

Association between Preoperative Retrograde Hepatic Vein Flow and Acute Kidney Injury after Cardiac Surgery
- PMID: 35328250
- PMCID: PMC8946915
- DOI: 10.3390/diagnostics12030699
Association between Preoperative Retrograde Hepatic Vein Flow and Acute Kidney Injury after Cardiac Surgery
Abstract
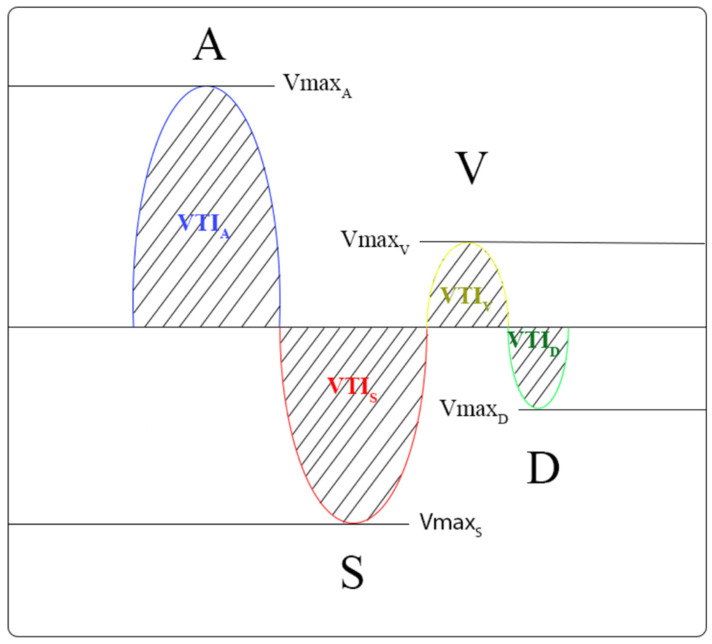
Key questions: Is there a predictive value of hepatic venous flow patterns for postoperative acute kidney injury (AKI) after cardiac surgery? Key findings: In patients who underwent cardiac surgery, retrograde hepatic venous waves (A, V) and their respective ratio to anterograde waves showed a strong association with postoperative AKI, defined as the percentage change of the highest postoperative serum creatinine from the baseline preoperative concentration (%ΔCr). The velocity time integral (VTI) of the retrograde A wave and the ratio of the retrograde and anterograde waves’ VTI were independently associated with AKI after adjustment for disease severity. Take-home message: A higher ratio of retrograde/antegrade waves in hepatic venous retrograde waves, which are related to hepatic stasis, may predict AKI after cardiac surgery. Introduction: Hepatic venous flow patterns reflect pressure changes in the right ventricle and are also markers of systemic venous congestion. Pulsatility of the inferior caval vein was used to predict the risk of acute kidney injury (AKI) after cardiac surgery. Aims: Our objective was to evaluate the association between preoperative hepatic venous flow patterns and the risk of AKI in patients after cardiac surgery. Methods: This prospective, observational study included 98 patients without preexisting liver disease who underwent cardiac surgery between 1 January 2018, and 31 March 2020, at a tertiary heart center. In addition to a routine echocardiographic examination, we recorded the maximal velocity and velocity time integral (VTI) of the standard four waves in the common hepatic vein with Doppler ultrasound. Our primary outcome measure was postoperative AKI, defined as the percentage change of the highest postoperative serum creatinine from the baseline preoperative concentration (%ΔCr). The secondary outcome was AKI, defined by KDIGO (Kidney Disease Improving Global Outcomes) criteria. Results: The median age of the patients was 69.8 years (interquartile range [IQR 25−75] 13 years). Seventeen patients (17.3%) developed postoperative AKI based on the KDIGO. The VTI of the retrograde A waves in the hepatic veins showed a strong correlation (B: 0.714; p = 0.0001) with an increase in creatinine levels after cardiac surgery. The velocity time integral (VTI) of the A wave (B = 0.038, 95% CI = 0.025−0.051, p < 0.001) and the ratio of VTI of the retrograde and anterograde waves (B = 0.233, 95% CI = 0.112−0.356, p < 0.001) were independently associated with an increase in creatinine levels. Conclusions: The severity of hepatic venous regurgitation can be a sign of venous congestion and seems to be related to the development of AKI.
Keywords: acute kidney injury; doppler ultrasound; heart failure; hepatic venous flow.
Conflict of interest statement
The authors declare no conflict of interest.
Figures



Similar articles
-
Association between Hepatic Venous Congestion and Adverse Outcomes after Cardiac Surgery.Diagnostics (Basel). 2022 Dec 15;12(12):3175. doi: 10.3390/diagnostics12123175. Diagnostics (Basel). 2022. PMID: 36553182 Free PMC article.
-
Ultrasound Hepatic Vein Ratios Are Associated With the Development of Acute Kidney Injury After Cardiac Surgery.J Cardiothorac Vasc Anesth. 2022 May;36(5):1326-1335. doi: 10.1053/j.jvca.2021.07.039. Epub 2021 Jul 28. J Cardiothorac Vasc Anesth. 2022. PMID: 34419361
-
Alterations in Portal Vein Flow and Intrarenal Venous Flow Are Associated With Acute Kidney Injury After Cardiac Surgery: A Prospective Observational Cohort Study.J Am Heart Assoc. 2018 Oct 2;7(19):e009961. doi: 10.1161/JAHA.118.009961. J Am Heart Assoc. 2018. PMID: 30371304 Free PMC article.
-
Doppler-based evaluation of intrarenal venous flow as a new tool to predict acute kidney injury: A systematic review and meta-analysis.Nefrologia (Engl Ed). 2023 Dec;43 Suppl 2:57-66. doi: 10.1016/j.nefroe.2023.05.010. Epub 2024 Jan 19. Nefrologia (Engl Ed). 2023. PMID: 38245439
-
Venous Doppler to Assess Congestion: A Comprehensive Review of Current Evidence and Nomenclature.Ultrasound Med Biol. 2023 Jan;49(1):3-17. doi: 10.1016/j.ultrasmedbio.2022.07.011. Epub 2022 Oct 4. Ultrasound Med Biol. 2023. PMID: 36207224 Review.
Cited by
-
Association between Hepatic Venous Congestion and Adverse Outcomes after Cardiac Surgery.Diagnostics (Basel). 2022 Dec 15;12(12):3175. doi: 10.3390/diagnostics12123175. Diagnostics (Basel). 2022. PMID: 36553182 Free PMC article.
-
Special Issue on "Advances in Image-Guided Diagnosis and Treatment of Abdominal Diseases".Diagnostics (Basel). 2023 Jan 4;13(2):169. doi: 10.3390/diagnostics13020169. Diagnostics (Basel). 2023. PMID: 36672979 Free PMC article.
-
The Preventive Role of Glutamine Supplementation in Cardiac Surgery-Associated Kidney Injury from Experimental Research to Clinical Practice: A Narrative Review.Medicina (Kaunas). 2024 May 3;60(5):761. doi: 10.3390/medicina60050761. Medicina (Kaunas). 2024. PMID: 38792944 Free PMC article. Review.
-
Diagnosis, pathophysiology and preventive strategies for cardiac surgery-associated acute kidney injury: a narrative review.Eur J Med Res. 2023 Jan 24;28(1):45. doi: 10.1186/s40001-023-00990-2. Eur J Med Res. 2023. PMID: 36694233 Free PMC article. Review.
References
-
- Petäjä L., Vaara S., Liuhanen S., Suojaranta-Ylinen R., Mildh L., Nisula S., Korhonen A.-M., Kaukonen K.-M., Salmenperä M., Pettilä V. Acute Kidney Injury after Cardiac Surgery by Complete KDIGO Criteria Predicts Increased Mortality. J. Cardiothorac. Vasc. Anesth. 2017;31:827–836. doi: 10.1053/j.jvca.2016.08.026. - DOI - PubMed
-
- Szyguła-Jurkiewicz B., Nadziakiewicz P., Zakliczynski M., Szczurek W., Chraponski J., Zembala M., Gasior M. Predictive Value of Hepatic and Renal Dysfunction Based on the Models for End-Stage Liver Disease in Patients with Heart Failure Evaluated for Heart Transplant. Transplant. Proc. 2016;48:1756–1760. doi: 10.1016/j.transproceed.2016.01.079. - DOI - PubMed
-
- Fuhrmann V., Kneidinger N., Herkner H., Heinz G., Nikfardjam M., Bojic A., Schellongowski P., Angermayr B., Kitzberger R., Warszawska J., et al. Hypoxic hepatitis: Underlying conditions and risk factors for mortality in critically ill patients. Intensive Care Med. 2009;35:1397–1405. doi: 10.1007/s00134-009-1508-2. - DOI - PubMed
-
- Farr M., Mitchell J., Lippel M., Kato T.S., Jin Z., Ippolito P., Dove L., Jorde U.P., Takayama H., Emond J., et al. Combination of liver biopsy with MELD-XI scores for post-transplant outcome prediction in patients with advanced heart failure and suspected liver dysfunction. J. Heart Lung Transplant. 2015;34:873–882. doi: 10.1016/j.healun.2014.12.009. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
