

Primary Effusion Lymphoma: A Timely Review on the Association with HIV, HHV8, and EBV
- PMID: 35328266
- PMCID: PMC8947353
- DOI: 10.3390/diagnostics12030713
Primary Effusion Lymphoma: A Timely Review on the Association with HIV, HHV8, and EBV
Abstract
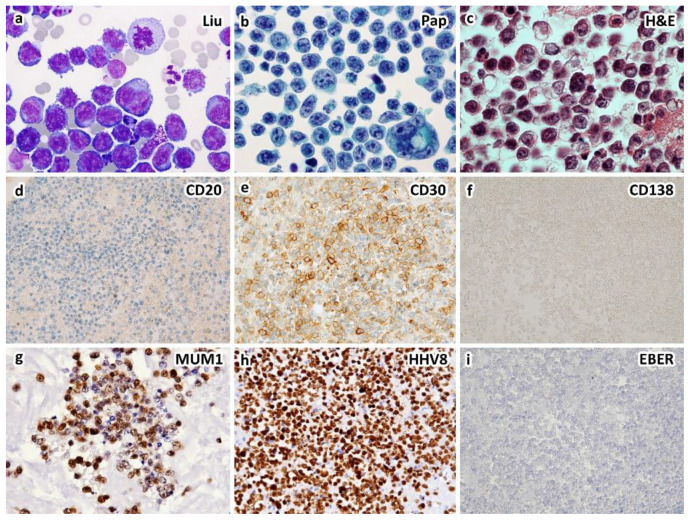
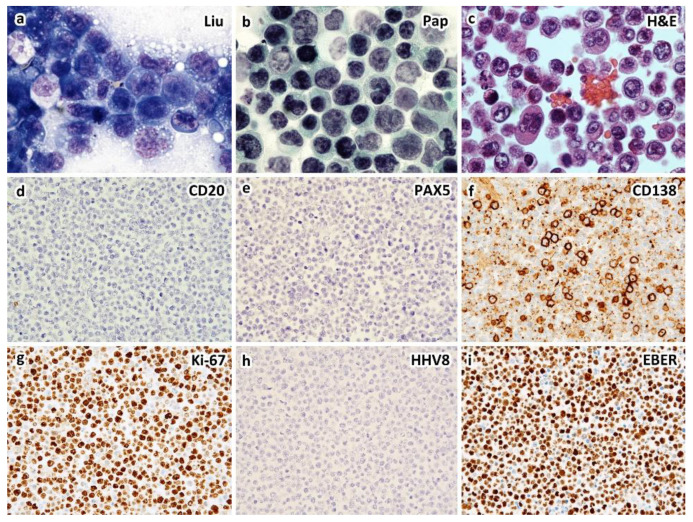
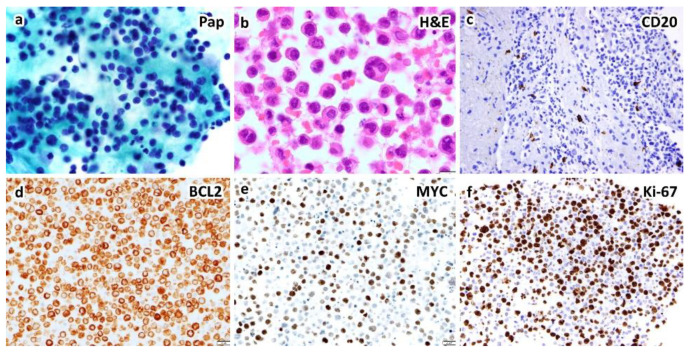
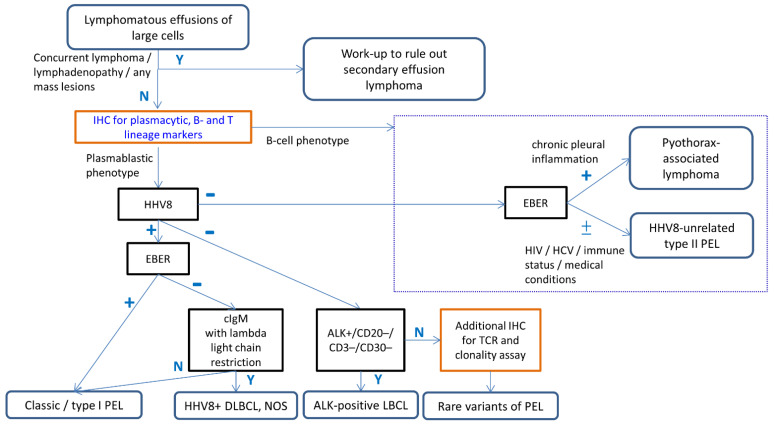
Primary effusion lymphoma (PEL) is defined by the WHO classification as a large B-cell neoplasm without detectable tumor masses. It is universally associated with HHV8, with most cases occurring in the setting of immunodeficiency such as HIV infection, and a poor prognosis. Morphologically, the neoplastic cells range from immunoblastic, plasmablastic, to anaplastic; and phenotypically, most cases express plasma cell but not B-cell markers, i.e., plasmablastic. During the past decade, primary HHV8-negative effusion lymphoma has been reported. Such cases were considered in the WHO classification scheme as effusion-based lymphoma. We performed a systemic review of 167 HHV8-negative effusion lymphomas from the literature and found that only 42% were associated with a fluid overload state, and with low rates of HIV (6%) or EBV (21%) infection. Furthermore, most patients are old (or immunosenescent) with underlying medical conditions/comorbidities, most neoplasms are of B-cell phenotype, and the outcome is more favorable than that of HHV8-positive PEL. These distinctive findings supported our prior proposal of designating these HHV8-negative cases as type II PEL, in contrast to the classic or type I PEL as defined by the WHO. Furthermore, we propose an algorithmic approach for the diagnosis of PEL and its mimickers.
Keywords: EBV; HHV8; HIV; effusion-based lymphoma; primary effusion lymphoma.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Primary effusion lymphoma in Taiwan shows two distinctive clinicopathological subtypes with rare human immunodeficiency virus association.Histopathology. 2018 May;72(6):930-944. doi: 10.1111/his.13449. Epub 2018 Feb 14. Histopathology. 2018. PMID: 29206290
-
Current concepts in primary effusion lymphoma and other effusion-based lymphomas.Korean J Pathol. 2014 Apr;48(2):81-90. doi: 10.4132/KoreanJPathol.2014.48.2.81. Epub 2014 Apr 28. Korean J Pathol. 2014. PMID: 24868220 Free PMC article. Review.
-
Extracavitary/solid variant of primary effusion lymphoma presenting as a gastric mass.Exp Mol Pathol. 2015 Dec;99(3):445-8. doi: 10.1016/j.yexmp.2015.09.010. Epub 2015 Sep 25. Exp Mol Pathol. 2015. PMID: 26407759
-
Primary Effusion Lymphoma: A Clinicopathological Study of 70 Cases.Cancers (Basel). 2021 Feb 19;13(4):878. doi: 10.3390/cancers13040878. Cancers (Basel). 2021. PMID: 33669719 Free PMC article.
-
Human Herpesvirus Type 8-associated Large B-cell Lymphoma: A Nonserous Extracavitary Variant of Primary Effusion Lymphoma in an HIV-infected Man: A Case Report and Review of the Literature.Clin Lymphoma Myeloma Leuk. 2016 Jun;16(6):311-21. doi: 10.1016/j.clml.2016.03.013. Epub 2016 Apr 1. Clin Lymphoma Myeloma Leuk. 2016. PMID: 27234438 Free PMC article. Review.
Cited by
-
Targeting VEGF with bevacizumab inhibits malignant effusion formation of primary human herpesvirus 8-unrelated effusion large B-cell lymphoma in vivo.J Cell Mol Med. 2022 Nov;26(22):5580-5589. doi: 10.1111/jcmm.17570. Epub 2022 Oct 9. J Cell Mol Med. 2022. PMID: 36209502 Free PMC article.
-
Cavity-based lymphomas: challenges and novel concepts. A report of the 2022 EA4HP/SH lymphoma workshop.Virchows Arch. 2023 Sep;483(3):299-316. doi: 10.1007/s00428-023-03599-2. Epub 2023 Aug 9. Virchows Arch. 2023. PMID: 37555981 Free PMC article.
-
Primary Effusion Lymphoma, Multicentric Castleman's Disease, and Kaposi's Sarcoma in an HHV-8 and HIV-Positive Patient: A Case Report.Medicina (Kaunas). 2023 May 30;59(6):1049. doi: 10.3390/medicina59061049. Medicina (Kaunas). 2023. PMID: 37374253 Free PMC article.
-
5-AZA Upregulates SOCS3 and PTPN6/SHP1, Inhibiting STAT3 and Potentiating the Effects of AG490 against Primary Effusion Lymphoma Cells.Curr Issues Mol Biol. 2024 Mar 14;46(3):2468-2479. doi: 10.3390/cimb46030156. Curr Issues Mol Biol. 2024. PMID: 38534772 Free PMC article.
-
The 'Oma's of the Gammas-Cancerogenesis by γ-Herpesviruses.Viruses. 2024 Dec 17;16(12):1928. doi: 10.3390/v16121928. Viruses. 2024. PMID: 39772235 Free PMC article. Review.
References
-
- Das D.K., Al-Juwaiser A., George S.S., Francis I.M., Sathar S.S., Sheikh Z.A., Shaheen A., Pathan S.K., Haji B.E., George J., et al. Cytomorphological and immunocytochemical study of non-Hodgkin’s lymphoma in pleural effusion and ascitic fluid. Cytopathology. 2007;18:157–167. doi: 10.1111/j.1365-2303.2007.00448.x. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
