

Effectiveness and Safety of Real-Time Transthoracic Ultrasound-Guided Thoracentesis
- PMID: 35328278
- PMCID: PMC8946970
- DOI: 10.3390/diagnostics12030725
Effectiveness and Safety of Real-Time Transthoracic Ultrasound-Guided Thoracentesis
Abstract
Purpose: The purpose of the present study was to specifically evaluate the effectiveness and safety of real-time ultrasound-guided thoracentesis in a case series of pleural effusion.
Patients and methods: An observational prospective study was conducted. From February 2018 to December 2019, a total of 361 consecutive real-time transthoracic ultrasound (TUS)-guided thoracentesis were performed in the Unit of Diagnostic and Interventional Ultrasound of the Research Hospital "Fondazione Casa Sollievo della Sofferenza" of San Giovanni Rotondo, Foggia, Italy. The primary indication for thoracentesis was therapeutic in all the cases (i.e., evacuation of persistent small/moderate pleural effusions to avoid super-infection; drainage of symptomatic moderate/massive effusions). For completeness, further diagnostic investigations (including chemical, microbiological, and cytological analysis) were conducted. All the procedures were performed by two internists with more than 30 years of experience in interventional ultrasound using a multifrequency convex probe (3-8 MHz). For pleural effusions with a depth of 2-3 cm measured at the level of the costo-phrenic sinus was employed a dedicated holed convex-array probe (5 MHz).
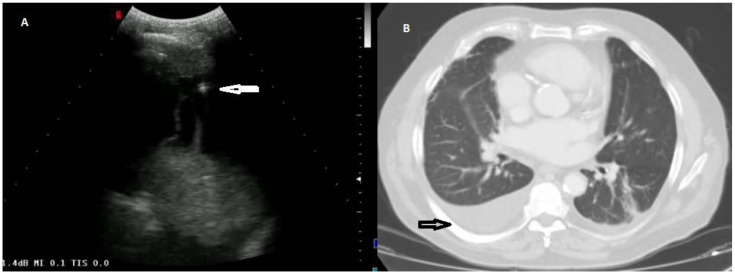
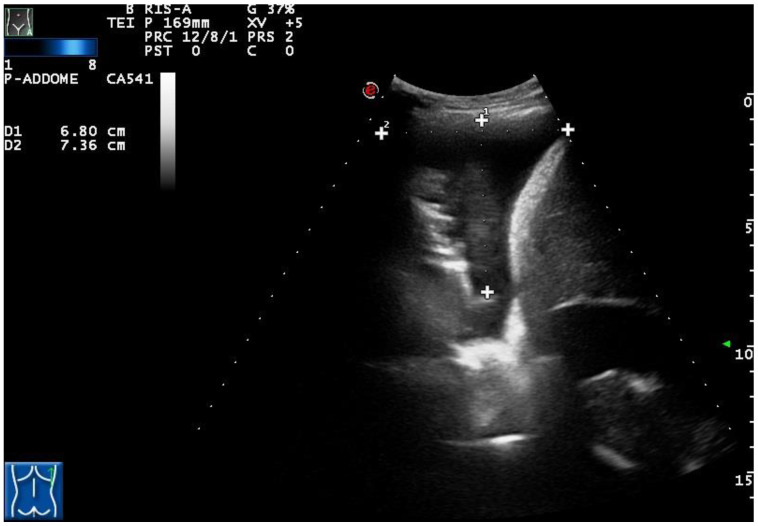
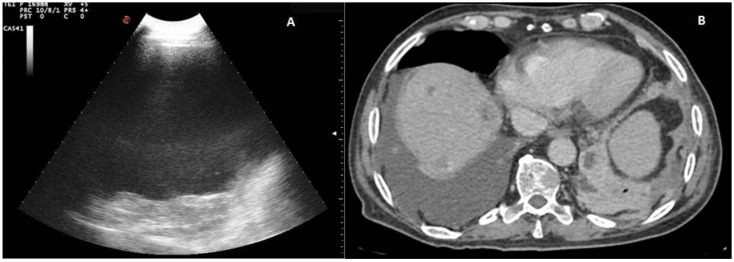
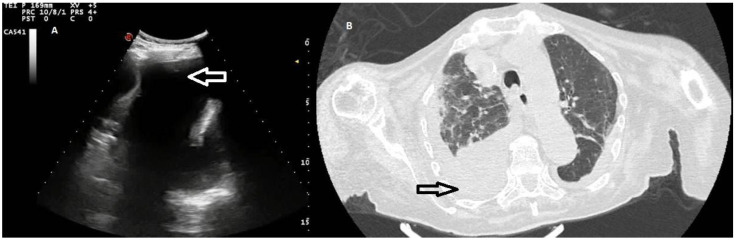
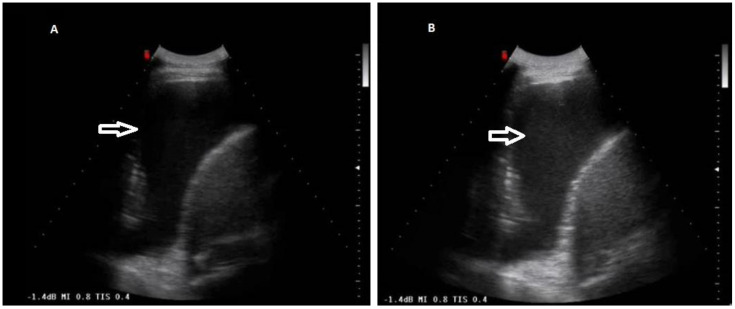
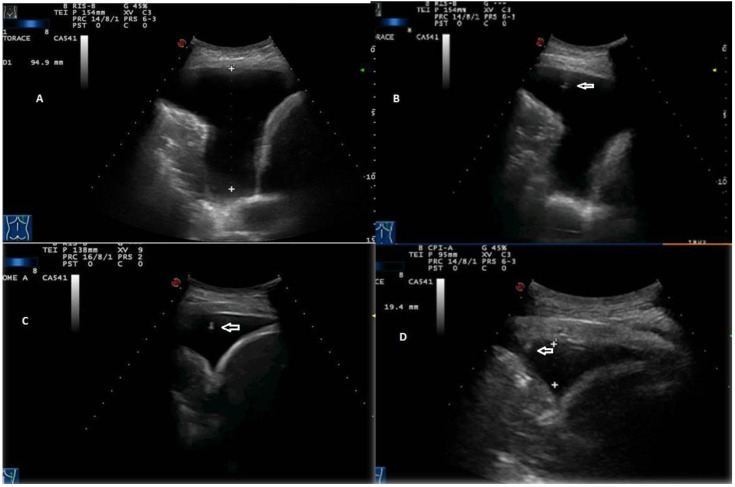
Results: In all the cases, the attempts at thoracentesis were successful, allowing the achievement of the therapeutic purpose of the procedure (i.e., the complete drying of the pleural space or the withdrawal of fluid till a "safe" quantity [a mean of 1.5 L, max 2 L] producing relief from symptoms) regardless of the initial extent of the pleural effusion. There were only 3 cases of pneumothorax, for a prevalence rate of complications in this population of 0.83%. No statistical difference was recorded in the rate of pneumothorax according to the initial amount of pleural fluid in the effusion (p = 0.12). All the pleural effusions classified as transudates showed an anechoic TUS appearance. Only the exudative effusions showed a complex nonseptated or a hyperechoic TUS appearance. However, an anechoic TUS pattern was not unequivocally associated with transudates. Some chronic transudates have been classified as exudates by Light's criteria, showing also a complex nonseptated TUS appearance. The cytological examination of the drained fluid allowed the detection of neoplastic cells in 15.89% cases. On the other hand, the microbiological examination of effusions yielded negative results in all the cases.
Conclusions: Real-time TUS-guided thoracentesis is a therapeutically effective and safe procedure, despite the diagnostic yield of the cytological or microbiological examinations on the collected liquid being very low. Future blinded randomized studies are required to definitely clarify the actual benefit of the real-time TUS-guided procedure over percussion-guided and other ultrasound-based procedures.
Keywords: effectiveness; pleural effusion; safety; transthoracic ultrasound; transthoracic ultrasound-guided thoracentesis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Similar articles
-
Diagnostic Accuracy of Thoracic Ultrasonography to Differentiate Transudative From Exudative Pleural Effusion.Chest. 2020 Aug;158(2):692-697. doi: 10.1016/j.chest.2020.02.051. Epub 2020 Mar 17. Chest. 2020. PMID: 32194059
-
The Use of Thoracic Ultrasound to Predict Transudative and Exudative Pleural Effusion.POCUS J. 2021 Nov 23;6(2):97-102. doi: 10.24908/pocus.v6i2.15193. eCollection 2021. POCUS J. 2021. PMID: 36895667 Free PMC article.
-
Pleural effusions in febrile medical ICU patients: chest ultrasound study.Chest. 2004 Oct;126(4):1274-80. doi: 10.1378/chest.126.4.1274. Chest. 2004. PMID: 15486393
-
Use of lung ultrasound for the diagnosis and treatment of pleural effusion.Eur Rev Med Pharmacol Sci. 2022 Dec;26(23):8771-8776. doi: 10.26355/eurrev_202212_30548. Eur Rev Med Pharmacol Sci. 2022. PMID: 36524495 Review.
-
[Current diagnostic approach to pleural effusion].Pneumologie. 2004 Nov;58(11):777-90. doi: 10.1055/s-2004-830084. Pneumologie. 2004. PMID: 15534774 Review. German.
Cited by
-
Exploration of the feasibility of clinical application of phage treatment for multidrug-resistant Serratia marcescens-induced pulmonary infection.Emerg Microbes Infect. 2025 Dec;14(1):2451048. doi: 10.1080/22221751.2025.2451048. Epub 2025 Jan 15. Emerg Microbes Infect. 2025. PMID: 39764739 Free PMC article.
-
Real-time Ultrasound-guided Lumbar Puncture: A Comparison of Two Techniques Using Simulation.West J Emerg Med. 2025 May 20;26(3):737-742. doi: 10.5811/westjem.21163. West J Emerg Med. 2025. PMID: 40561993 Free PMC article. Clinical Trial.
-
Influence of age and sex on the diagnostic accuracy of pleural fluid carcinoembryonic antigen for malignant pleural effusion: a post hoc analysis.Front Oncol. 2025 May 6;15:1549621. doi: 10.3389/fonc.2025.1549621. eCollection 2025. Front Oncol. 2025. PMID: 40395336 Free PMC article.
-
First Reported Case of Iatrogenic Cardiac Tamponade Following Chest Drain Insertion for Tension Pneumothorax in a Premature Newborn.Case Rep Pediatr. 2025 May 18;2025:7960753. doi: 10.1155/crpe/7960753. eCollection 2025. Case Rep Pediatr. 2025. PMID: 40420844 Free PMC article.
-
New strategies in the management of pneumothorax.Breathe (Sheff). 2025 Aug 19;21(3):240250. doi: 10.1183/20734735.0250-2024. eCollection 2025 Jul. Breathe (Sheff). 2025. PMID: 40837422 Free PMC article. Review.
References
-
- Villena Garrido V., Cases Viedma E., Fernández Villar A., de Pablo Gafas A., Pérez Rodríguez E., Porcel Pérez J.M., Rodríguez Panadero F., Ruiz Martínez C., Salvatierra Velázquez Á., Valdés Cuadrado L. Recommendations of Diagnosis and Treatment of Pleural Effusion. Update. Arch. Bronconeumol. 2014;50:235–249. doi: 10.1016/j.arbres.2014.01.016. - DOI - PubMed
LinkOut - more resources
Full Text Sources
