

Intracranial Flow Volume Estimation in Patients with Internal Carotid Artery Occlusion
- PMID: 35328320
- PMCID: PMC8947284
- DOI: 10.3390/diagnostics12030766
Intracranial Flow Volume Estimation in Patients with Internal Carotid Artery Occlusion
Abstract
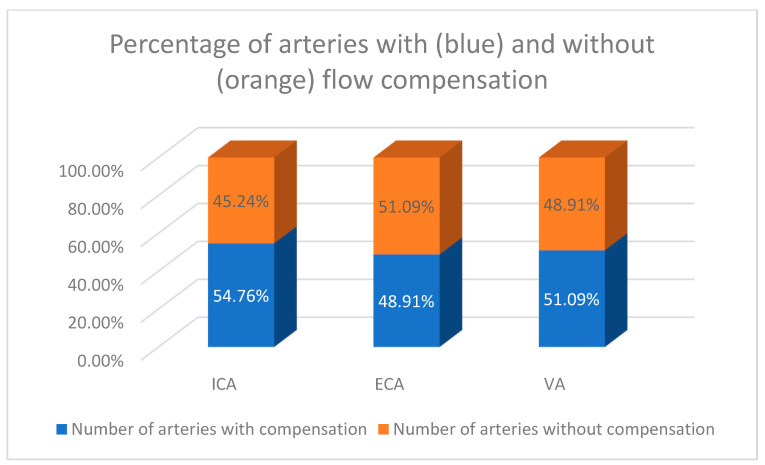
(1) Background: Carotid artery occlusion (CAO) in population studies has a reported prevalence of about 6 per 100,000 people; however, the data may be underestimated. CAO carries a significant risk of stroke. Up to 15% of large artery infractions may be secondary to the CAO, and in 27−38% of patients, ischaemic stroke is a first presentation of the disease. The presence of sufficient and well-developed collateral circulation has a protective influence, being a good prognostic factor in patients with carotid artery disease, both chronic and acute. Understanding the mechanisms and role of collateral circulation may be very important in the risk stratification of such patients. (2) Materials and Methods: This study included 46 patients (mean age: 70.5 ± 6 years old; 15 female, mean age 68.5 ± 3.8 years old and 31 male, mean age 71.5 ± 6.7 years old) with unilateral or bilateral ICA occlusion. In all patients, a Doppler ultrasound (DUS) examination, measuring blood flow volume in the internal carotid artery (ICA), external carotid artery (ECA), and vertebral artery (VA), was performed. The cerebral blood flow (CBF) was compared to the previously reported CBF values in the healthy population >65 years old. (3) Results: In comparison with CBF values in the healthy population, three subgroups with CBF changes were identified among patients with ICA occlusion: patients with significant volumetric flow compensation (CBF higher than average + standard deviation for healthy population of the same age), patients with flow similar to the healthy population (average ± standard deviation), and patients without compensation (CBF lower than the average-standard deviation for healthy population). The percentage of patients with significant volumetric flow compensation tend to rise with increasing age, while a simultaneous decline was observed in the group without compensation. The percentage of patients with flow similar to the healthy population remained relatively unchanged. ICA played the most important role in volumetric flow compensation in patients with CAO; however, the relative increase in flow in the ICA was smaller than that in the ECA and VA. Compensatory increased flow was observed in about 50% of all patent extracranial arteries and was more frequently observed in ipsilateral vessels than in contralateral ones, in both the ECA and the VA. In patients with CAO, there was no decrease in CBF, ICA, ECA, and VA flow volume with increasing age. (4) Conclusions: Volumetric flow compensation may play an important predictive role in patients with CAO.
Keywords: Doppler ultrasonography; carotid artery disease; carotid occlusion; cerebral blood flow; cerebrovascular reserve.
Conflict of interest statement
The authors declare no conflict of interest.
Figures










Similar articles
-
Impact of Internal Carotid Stenosis Treatment on Cerebral Blood Flow Volume: A Comparative Study between Preoperative and Postoperative Values.Med Sci Monit. 2023 Dec 10;29:e941958. doi: 10.12659/MSM.941958. Med Sci Monit. 2023. PMID: 38071424 Free PMC article.
-
Volumetric Flow Assessment in Extracranial Arteries in Patients with 70-99% Internal Carotid Artery Stenosis.Diagnostics (Basel). 2022 Sep 13;12(9):2216. doi: 10.3390/diagnostics12092216. Diagnostics (Basel). 2022. PMID: 36140616 Free PMC article.
-
Volumetric Flow Assessment in Doppler Ultrasonography in Risk Stratification of Patients with Internal Carotid Stenosis and Occlusion.J Clin Med. 2022 Jan 20;11(3):531. doi: 10.3390/jcm11030531. J Clin Med. 2022. PMID: 35159983 Free PMC article.
-
Volumetric Carotid Flow Characteristics in Doppler Ultrasonography in Healthy Population Over 65 Years Old.J Clin Med. 2020 May 7;9(5):1375. doi: 10.3390/jcm9051375. J Clin Med. 2020. PMID: 32392788 Free PMC article.
-
The critical role of the external carotid artery in cerebral perfusion of patients with total occlusion of the internal carotid artery.Int Angiol. 2012 Feb;31(1):16-21. Int Angiol. 2012. PMID: 22330620
Cited by
-
Accuracy of Computed Tomography Angiography for Diagnosing Extracranial Mural Lesions in Patients with Acute Internal Carotid Artery Occlusion: Correlation with Digital Subtraction Angiography.J Pers Med. 2023 Jul 21;13(7):1169. doi: 10.3390/jpm13071169. J Pers Med. 2023. PMID: 37511782 Free PMC article.
-
Branching and nonbranching intracranial aneurysms in the presence of a persistent stapedial artery and an aberrant internal carotid artery assessed with computational hemodynamics: illustrative case.J Neurosurg Case Lessons. 2024 Nov 4;8(19):CASE24421. doi: 10.3171/CASE24421. Print 2024 Nov 4. J Neurosurg Case Lessons. 2024. PMID: 39496146 Free PMC article.
-
Impact of Internal Carotid Stenosis Treatment on Cerebral Blood Flow Volume: A Comparative Study between Preoperative and Postoperative Values.Med Sci Monit. 2023 Dec 10;29:e941958. doi: 10.12659/MSM.941958. Med Sci Monit. 2023. PMID: 38071424 Free PMC article.
-
Volumetric Flow Assessment in Extracranial Arteries in Patients with 70-99% Internal Carotid Artery Stenosis.Diagnostics (Basel). 2022 Sep 13;12(9):2216. doi: 10.3390/diagnostics12092216. Diagnostics (Basel). 2022. PMID: 36140616 Free PMC article.
-
The Effect of Circle of Willis Morphology on Retinal Blood Flow in Patients with Carotid Stenosis Measured by Optical Coherence Tomography Angiography.J Clin Med. 2023 Aug 16;12(16):5335. doi: 10.3390/jcm12165335. J Clin Med. 2023. PMID: 37629376 Free PMC article.
References
-
- Sigvant B., Wiberg-Hedman K., Bergqvist D., Rolandsson O., Andersson B., Persson E., Wahlberg E. A population-based study of peripheral arterial disease prevalence with special focus on critical limb ischemia and sex differences. J. Vasc. Surg. 2007;45:1185–1191. doi: 10.1016/j.jvs.2007.02.004. - DOI - PubMed
-
- WHO: The Atlas of Heart Disease and Stroke: Global Burden of Stroke. [(accessed on 28 May 2019)]. Available online: http://www.who.int/cardiovascular_diseases/resources/atlas/en.
LinkOut - more resources
Full Text Sources
Miscellaneous
