

The Significance of Epidermal Growth Factor in Noninvasively Obtained Amniotic Fluid Predicting Respiratory Outcomes of Preterm Neonates
- PMID: 35328399
- PMCID: PMC8953784
- DOI: 10.3390/ijms23062978
The Significance of Epidermal Growth Factor in Noninvasively Obtained Amniotic Fluid Predicting Respiratory Outcomes of Preterm Neonates
Abstract
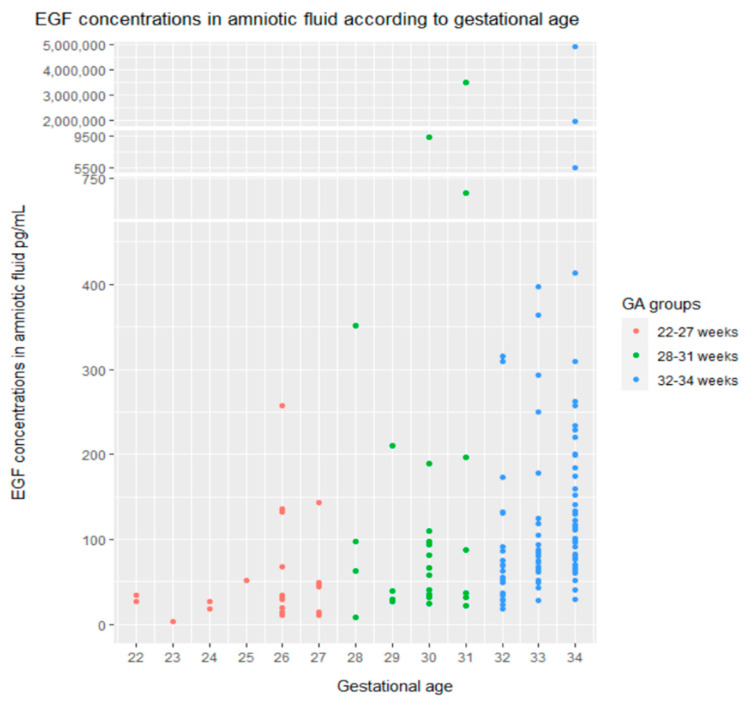
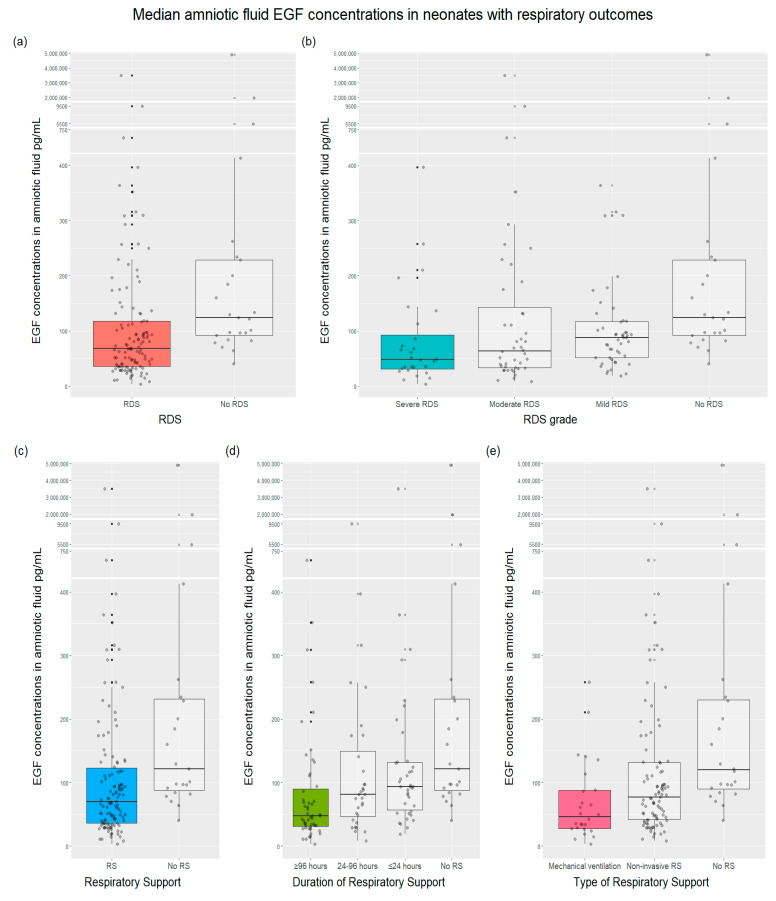
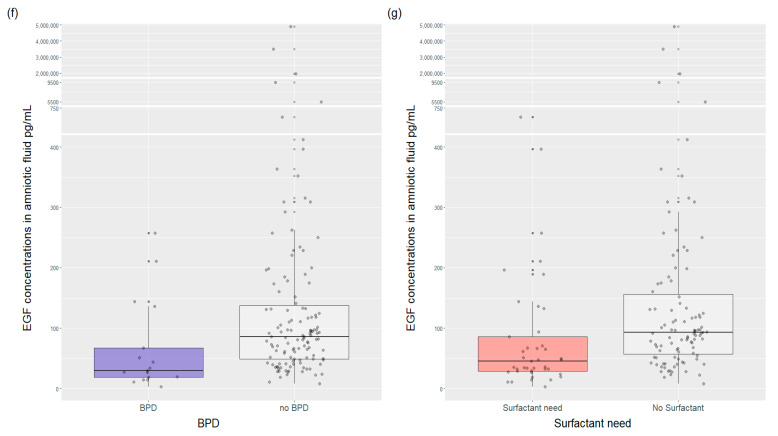
Preterm premature rupture of membranes (PPROM) interrupts normal lung development, resulting in neonatal respiratory morbidity. Although post-PPROM risks have been researched, only a few studies have investigated noninvasively obtained amniotic fluid (AF) to predict neonatal outcomes. In this study, we aimed to determine whether epidermal growth factor (EGF) in vaginally-collected AF is a significant predictor of neonatal respiratory outcomes after PPROM. We analyzed EGF in vaginally-obtained AF from 145 women with PPROM at 22−34 weeks of gestation. The following neonatal outcomes were included: respiratory distress syndrome, surfactant need, duration and type of respiratory support, and bronchopulmonary dysplasia. We found that EGF concentration was associated with gestational age, and its medians were lower in neonates with respiratory morbidities than unaffected ones. EGF concentrations gradually declined, the lowest being in the most clinically ill patients. EGF < 35 pg/mL significantly predicted the odds of severe respiratory outcomes. EGF in noninvasively collected AF may be a reliable predictor for respiratory outcomes of preterm neonates with PPROM before 34 weeks of gestation. The results of our study may have implications for further research both in noninvasive amniotic fluid analysis and the management of patients after PPROM.
Keywords: amniotic fluid; epidermal growth factor; noninvasive method; preterm birth; preterm premature rupture of membranes; respiratory outcomes.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study, in the collection, analyses, or interpretation of data, in the writing of the manuscript, or in the decision to publish the results.
Figures
Similar articles
-
Phenotypic overlap in neonatal respiratory morbidity following preterm premature rupture of membranes versus spontaneous preterm labor.J Matern Fetal Neonatal Med. 2021 Jun;34(12):1941-1948. doi: 10.1080/14767058.2019.1651280. Epub 2019 Aug 11. J Matern Fetal Neonatal Med. 2021. PMID: 31402735 Free PMC article.
-
Amniotic fluid volume at presentation with early preterm prelabor rupture of membranes and association with severe neonatal respiratory morbidity.Ultrasound Obstet Gynecol. 2019 Dec;54(6):767-773. doi: 10.1002/uog.20257. Ultrasound Obstet Gynecol. 2019. PMID: 30834608
-
Comparison between maternal and neonatal outcome of PPROM in the cases of amniotic fluid index (AFI) of more and less than 5 cm.J Obstet Gynaecol. 2018 Jul;38(5):611-615. doi: 10.1080/01443615.2017.1394280. Epub 2018 Feb 9. J Obstet Gynaecol. 2018. PMID: 29426264
-
Mid-trimester preterm premature rupture of membranes (PPROM): etiology, diagnosis, classification, international recommendations of treatment options and outcome.J Perinat Med. 2018 Jul 26;46(5):465-488. doi: 10.1515/jpm-2017-0027. J Perinat Med. 2018. PMID: 28710882 Review.
-
Periviable Premature Rupture of Membranes.Obstet Gynecol Clin North Am. 2020 Dec;47(4):633-651. doi: 10.1016/j.ogc.2020.08.007. Epub 2020 Oct 7. Obstet Gynecol Clin North Am. 2020. PMID: 33121650 Review.
Cited by
-
Prediction of preeclampsia using maternal circulating mRNAs in early pregnancy.Arch Gynecol Obstet. 2024 Jul;310(1):327-335. doi: 10.1007/s00404-024-07486-2. Epub 2024 Apr 3. Arch Gynecol Obstet. 2024. PMID: 38568284
-
Evolutionary bridges: how factors present in amniotic fluid and human milk help mature the gut.J Perinatol. 2024 Nov;44(11):1552-1559. doi: 10.1038/s41372-024-02026-x. Epub 2024 Jun 6. J Perinatol. 2024. PMID: 38844520 Free PMC article. Review.
References
-
- Liu L., Oza S., Hogan D., Chu Y., Perin J., Zhu J., Lawn J.E., Cousens S., Mathers C., Black R.E. Global, Regional, and National Causes of under-5 Mortality in 2000–15: An Updated Systematic Analysis with Implications for the Sustainable Development Goals. Lancet. 2016;388:3027–3035. doi: 10.1016/S0140-6736(16)31593-8. - DOI - PMC - PubMed
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
