

Cell Therapy Based on Gingiva-Derived Mesenchymal Stem Cells Seeded in a Xenogeneic Collagen Matrix for Root Coverage of RT1 Gingival Lesions: An In Vivo Experimental Study
- PMID: 35328670
- PMCID: PMC8950013
- DOI: 10.3390/ijms23063248
Cell Therapy Based on Gingiva-Derived Mesenchymal Stem Cells Seeded in a Xenogeneic Collagen Matrix for Root Coverage of RT1 Gingival Lesions: An In Vivo Experimental Study
Abstract
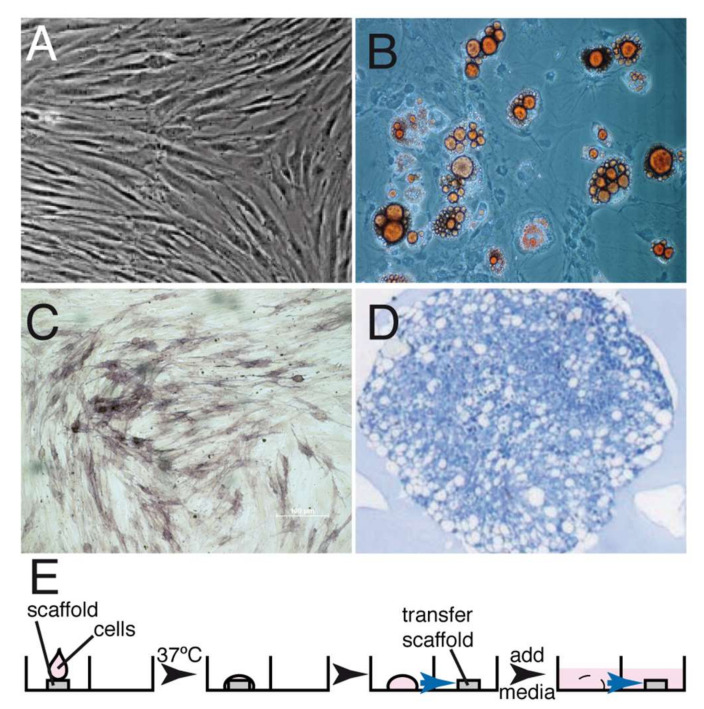
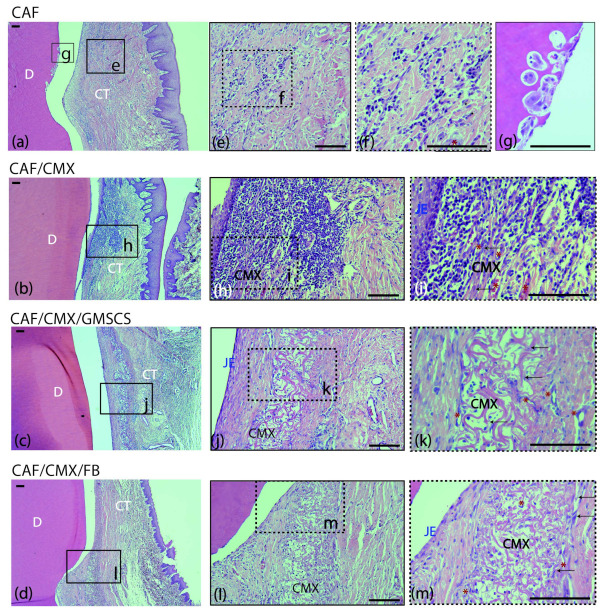
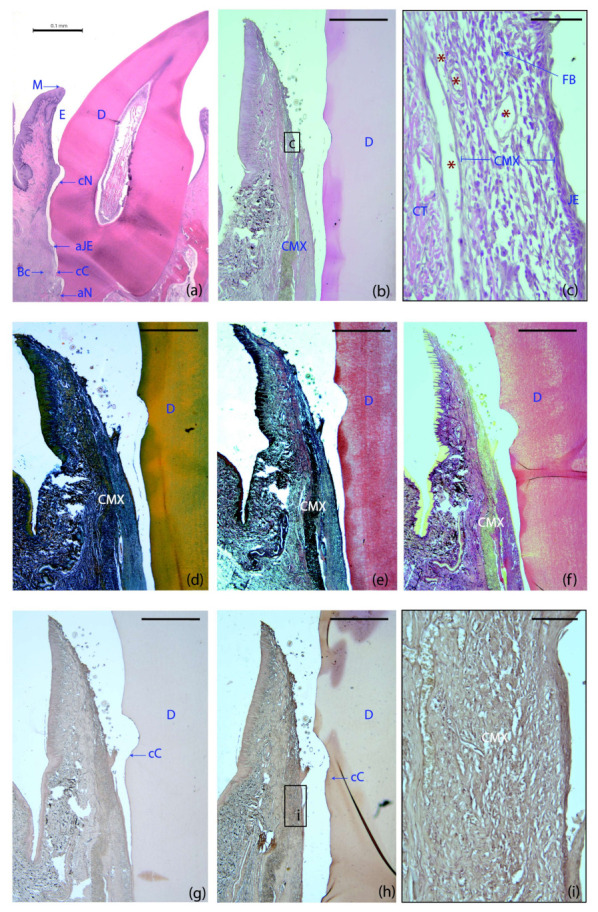
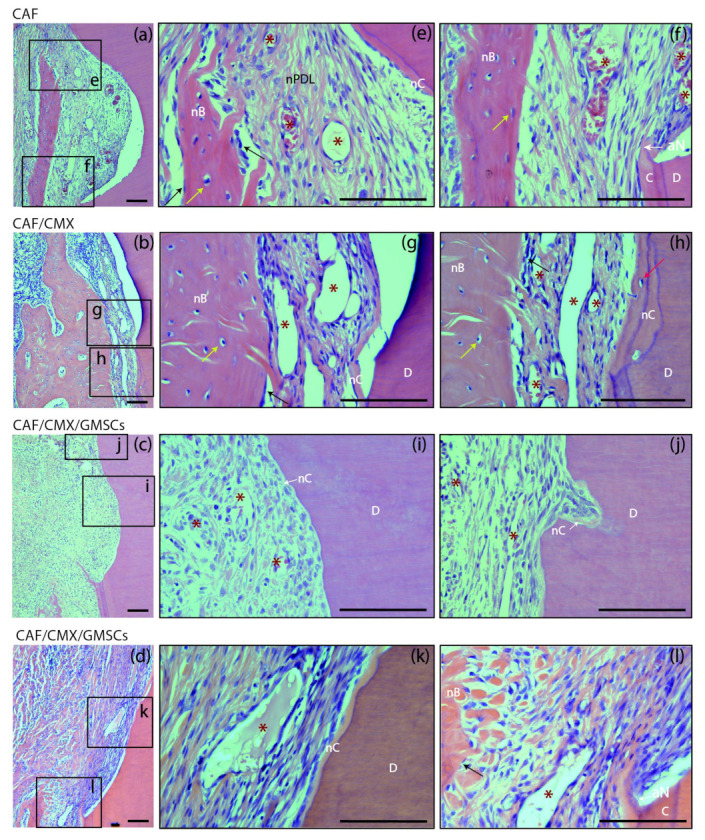
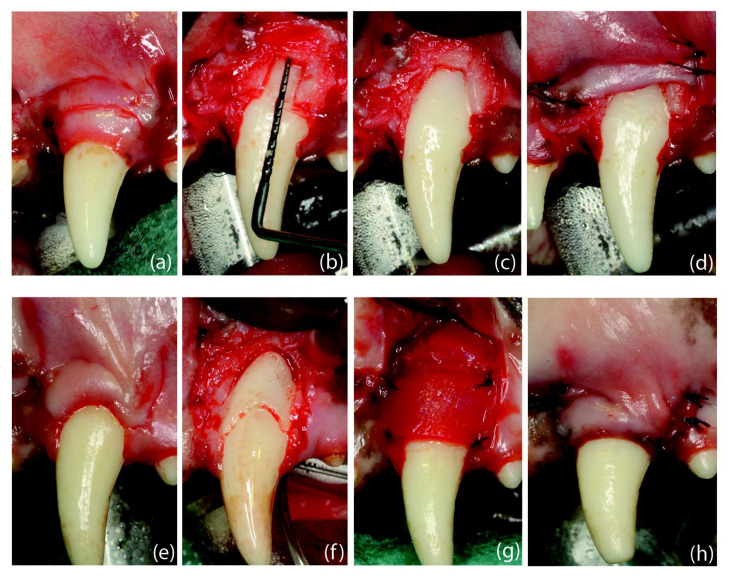
(1) Background: To investigate the effect of a xenogeneic collagen matrix (CMX) seeded with autologous gingiva-derived mesenchymal cells (GMSCs) when combined with a coronally advanced flap (CAF) in the treatment of localized gingival recession type 1 (RT1). (2) Methods: Dehiscence-type defects were created in seven dogs. GMSCs were isolated, transfected with a vector carrying green fluorescent protein (GFP) and expanded. Once chronified, the defects were randomly treated with (1) CAF plus the combination of CMX and GFP+ GMSCs, (2) CAF plus CMX with autologous fibroblasts, (3) CAF plus CMX and (4) CAF alone. Histological and clinical outcomes at 2- and 6-week healing periods were analyzed and compared among groups. (3) Results: Histologically, the addition of autologous cells to the CMX resulted in reduced inflammation and a variable degree of new cementum/bone formation. CMX plus GMSCs resulted in greater mean recession reduction (1.42; SD = 1.88 mm) and percentage of teeth with recession reduction of ≥2 mm (57%) when compared to the other groups, although these differences were not statistically significant. (4) Conclusions: The histometric and clinical results indicated a positive trend favouring the combination of CMX and GMSCs with the CAF when compared to the groups without cells, although these differences were not statistically significant.
Keywords: cell therapy; gingiva-derived stem cells; gingival recession; mesenchymal stem cells; mesenchymal stromal cells; root coverage; soft tissue regeneration.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
Similar articles
-
Xenogeneic collagen matrix with coronally advanced flap compared to connective tissue with coronally advanced flap for the treatment of dehiscence-type recession defects.J Periodontol. 2010 Aug;81(8):1108-17. doi: 10.1902/jop.2010.090698. J Periodontol. 2010. PMID: 20350159 Clinical Trial.
-
Healing of buccal gingival recessions following treatment with coronally advanced flap alone or combined with a cross-linked hyaluronic acid gel. An experimental study in dogs.J Clin Periodontol. 2021 Apr;48(4):570-580. doi: 10.1111/jcpe.13433. Epub 2021 Feb 10. J Clin Periodontol. 2021. PMID: 33513277 Free PMC article.
-
Long-Term Results Comparing Xenogeneic Collagen Matrix and Autogenous Connective Tissue Grafts With Coronally Advanced Flaps for Treatment of Dehiscence-Type Recession Defects.J Periodontol. 2016 Mar;87(3):221-7. doi: 10.1902/jop.2015.150386. Epub 2015 Oct 15. J Periodontol. 2016. PMID: 26469812 Clinical Trial.
-
Periodontal soft tissue root coverage procedures: a consensus report from the AAP Regeneration Workshop.J Periodontol. 2015 Feb;86(2 Suppl):S52-5. doi: 10.1902/jop.2015.140376. Epub 2014 Oct 15. J Periodontol. 2015. PMID: 25315018
-
Clinical efficacy of xenogeneic collagen matrix in the treatment of gingival recession: a systematic review and meta-analysis.Acta Odontol Scand. 2019 Aug;77(6):457-467. doi: 10.1080/00016357.2019.1588372. Epub 2019 Mar 21. Acta Odontol Scand. 2019. PMID: 30896271
Cited by
-
Gingival mesenchymal stem cells: Biological properties and therapeutic applications.J Oral Biol Craniofac Res. 2024 Sep-Oct;14(5):547-569. doi: 10.1016/j.jobcr.2024.07.003. Epub 2024 Jul 13. J Oral Biol Craniofac Res. 2024. PMID: 39108352 Free PMC article.
-
Adult Mesenchymal Stem Cells from Oral Cavity and Surrounding Areas: Types and Biomedical Applications.Pharmaceutics. 2023 Aug 9;15(8):2109. doi: 10.3390/pharmaceutics15082109. Pharmaceutics. 2023. PMID: 37631323 Free PMC article. Review.
References
-
- Nunez J., Caffesse R., Vignoletti F., Guerra F., San Roman F., Sanz M. Clinical and histological evaluation of an acellular dermal matrix allograft in combination with the coronally advanced flap in the treatment of Miller class I recession defects: An experimental study in the mini-pig. J. Clin. Periodontol. 2009;36:523–531. doi: 10.1111/j.1600-051X.2009.01401.x. - DOI - PubMed
-
- Vignoletti F., Nunez J., Discepoli N., De Sanctis F., Caffesse R., Munoz F., Lopez M., Sanz M. Clinical and histological healing of a new collagen matrix in combination with the coronally advanced flap for the treatment of Miller class-I recession defects: An experimental study in the minipig. J. Clin. Periodontol. 2011;38:847–855. doi: 10.1111/j.1600-051X.2011.01767.x. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
