

Role of Extracellular High-Mobility Group Box-1 as a Therapeutic Target of Gastric Cancer
- PMID: 35328684
- PMCID: PMC8953630
- DOI: 10.3390/ijms23063264
Role of Extracellular High-Mobility Group Box-1 as a Therapeutic Target of Gastric Cancer
Abstract
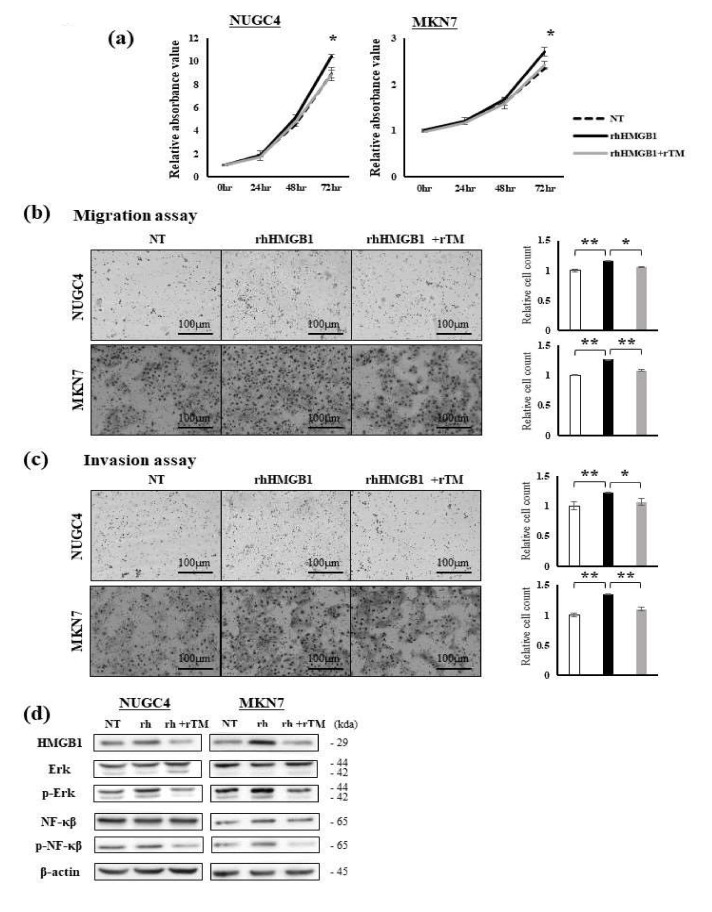
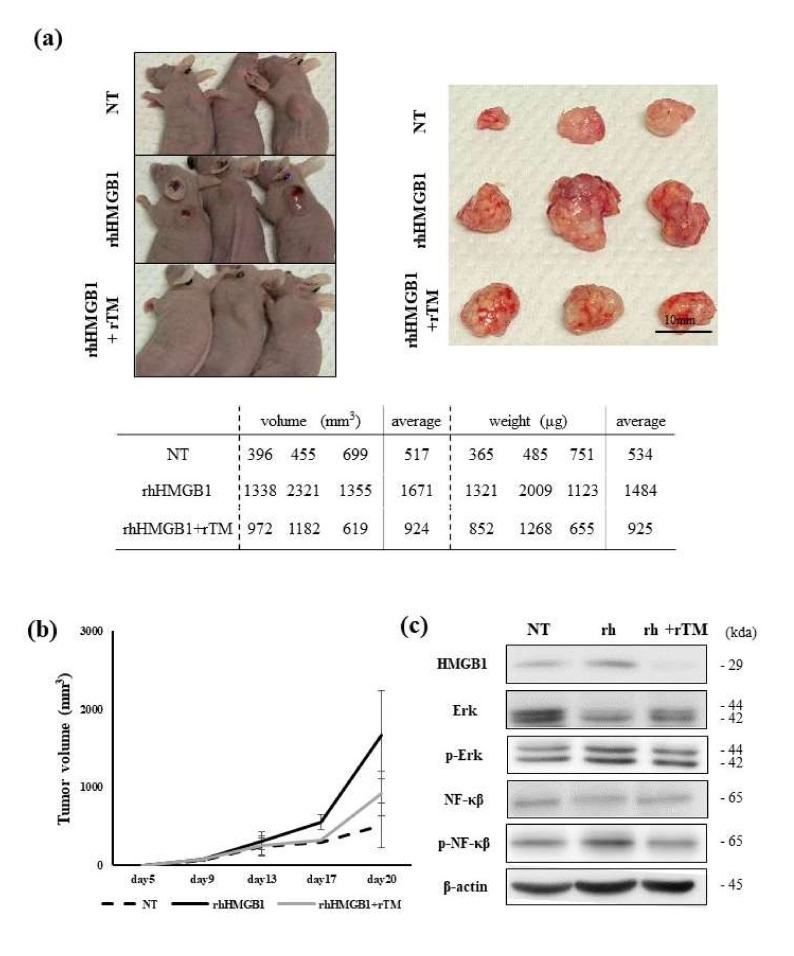
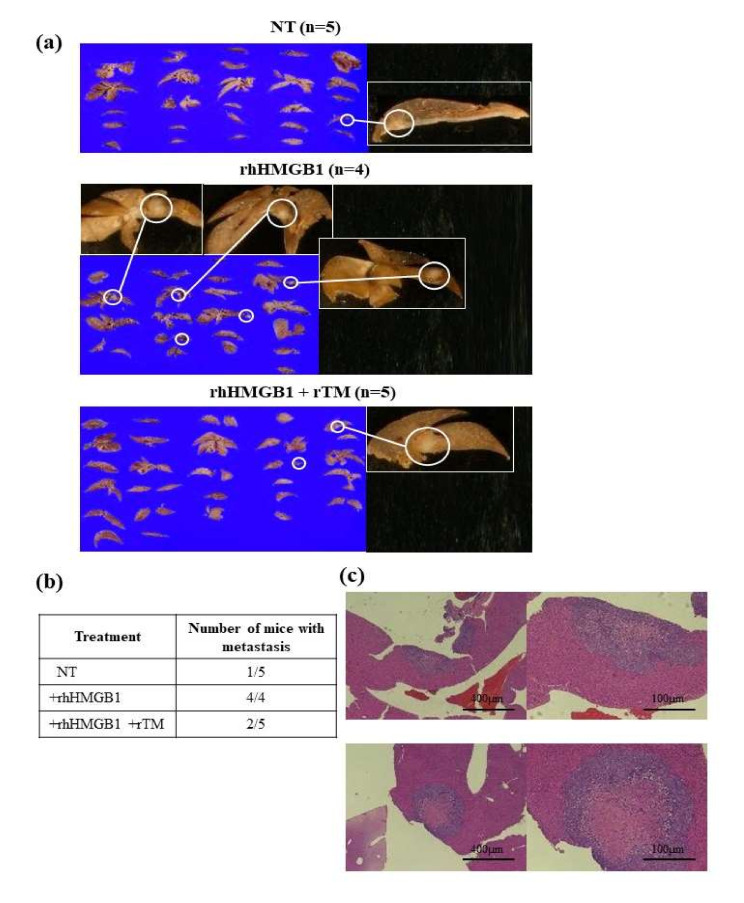
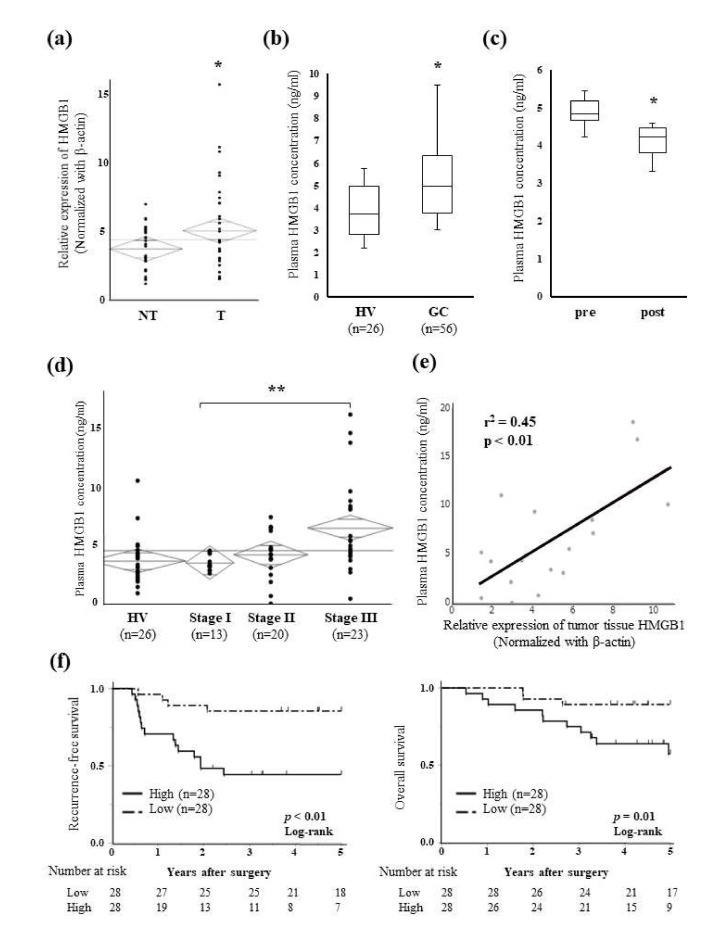
Background: High-mobility group box-1 (HMGB1) is involved in the tumorigenesis and metastasis of various cancers. The present study investigated the roles of extracellular HMGB1 in the progression of gastric cancer (GC) and the therapeutic effects of recombinant human soluble thrombomodulin (rTM) targeting HMGB1. Methods: The effects of extracellular HMGB1 and rTM on GC cells were assessed using proliferation and Transwell assays. Their effects on local tumor growth and metastasis were evaluated using subcutaneous tumor and liver metastasis mouse models, respectively. Plasma HMGB1 concentrations in GC patients were measured using ELISA. The relationships between plasma HMGB1 concentrations and the prognosis and clinicopathological factors of patients were also investigated. Results: GC proliferation, migration, and invasion abilities were promoted by increases in extracellular HMGB1 concentrations and alleviated by rTM. In the subcutaneous tumor model, local tumor growth was promoted by the addition of rhHMGB1 and alleviated by rTM. Similar changes occurred in the liver metastasis model. Recurrence-free survival (p < 0.01) and overall survival (p = 0.01) were significantly worse in patients with high plasma HMGB1 concentrations. Conclusion: Plasma HMGB1 concentrations are a prognostic marker in GC patients. Extracellular HMGB1 promotes cancer progression and has potential as a novel treatment target in GC cells for rTM.
Keywords: gastric cancer; high-mobility group box-1; recombinant human soluble thrombomodulin.
Conflict of interest statement
We declare no conflict of interest.
Figures
Similar articles
-
Combined targeting of high-mobility group box-1 and interleukin-8 to control micrometastasis potential in gastric cancer.Int J Cancer. 2015 Oct 1;137(7):1598-609. doi: 10.1002/ijc.29539. Epub 2015 Apr 16. Int J Cancer. 2015. PMID: 25821182
-
High-mobility group box-1 contributes tumor angiogenesis under interleukin-8 mediation during gastric cancer progression.Cancer Sci. 2017 Aug;108(8):1594-1601. doi: 10.1111/cas.13288. Epub 2017 Jul 7. Cancer Sci. 2017. PMID: 28574630 Free PMC article.
-
Specific detection of high mobility group box 1 degradation product with a novel ELISA.Mol Med. 2021 Jun 9;27(1):59. doi: 10.1186/s10020-021-00323-1. Mol Med. 2021. PMID: 34107884 Free PMC article.
-
Recombinant thrombomodulin ameliorates experimental autoimmune encephalomyelitis by suppressing high mobility group box 1 and inflammatory cytokines.Clin Exp Immunol. 2018 Jul;193(1):47-54. doi: 10.1111/cei.13123. Epub 2018 Mar 26. Clin Exp Immunol. 2018. PMID: 29509323 Free PMC article.
-
The implication and potential applications of high-mobility group box 1 protein in breast cancer.Ann Transl Med. 2016 Jun;4(11):217. doi: 10.21037/atm.2016.05.36. Ann Transl Med. 2016. PMID: 27386491 Free PMC article. Review.
Cited by
-
The mechanism of high mobility group box-1 protein and its bidirectional regulation in tumors.Biomol Biomed. 2024 May 2;24(3):477-485. doi: 10.17305/bb.2023.9760. Biomol Biomed. 2024. PMID: 37897664 Free PMC article. Review.
-
The Multifaceted Roles of Thrombomodulin: Anti-coagulation, Anti-inflammation, and Anti-tumor Potential.Curr Pharm Des. 2025;31(21):1673-1682. doi: 10.2174/0113816128335289241218161938. Curr Pharm Des. 2025. PMID: 39901541 Review.
-
Function of hsa_circ_0006646 as a competing endogenous RNA to promote progression in gastric cancer by regulating the miR-665-HMGB1 axis.J Gastrointest Oncol. 2023 Jun 30;14(3):1259-1278. doi: 10.21037/jgo-23-240. Epub 2023 May 15. J Gastrointest Oncol. 2023. PMID: 37435216 Free PMC article.
-
Obesity paradox as a new insight from postoperative complications in gastric cancer.Sci Rep. 2023 Jun 21;13(1):10116. doi: 10.1038/s41598-023-36968-7. Sci Rep. 2023. PMID: 37344511 Free PMC article.
-
A Novel Telomere Maintenance Gene-Related Model for Prognosis Prediction in Gastric Cancer.Biochem Genet. 2025 May 20. doi: 10.1007/s10528-025-11132-0. Online ahead of print. Biochem Genet. 2025. PMID: 40392448
References
-
- Sano T., Coit D.G., Kim H.H., Roviello F., Kassab P., Wittekind C., Yamamoto Y., Ohashi Y. Proposal of a new stage grouping of gastric cancer for TNM classification: International Gastric Cancer Association staging project. Gastric Cancer. 2017;20:217–225. doi: 10.1007/s10120-016-0601-9. - DOI - PMC - PubMed
-
- Chen L.-T., Satoh T., Ryu M.-H., Chao Y., Kato K., Chung H.C., Chen J.-S., Muro K., Kang W.K., Yeh K.-H., et al. A phase 3 study of nivolumab in previously treated advanced gastric or gastroesophageal junction cancer (ATTRACTION-2): 2-year update data. Gastric Cancer. 2020;23:510–519. doi: 10.1007/s10120-019-01034-7. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
