

Autosomal Dominant Polycystic Kidney Disease: From Pathophysiology of Cystogenesis to Advances in the Treatment
- PMID: 35328738
- PMCID: PMC8949594
- DOI: 10.3390/ijms23063317
Autosomal Dominant Polycystic Kidney Disease: From Pathophysiology of Cystogenesis to Advances in the Treatment
Abstract
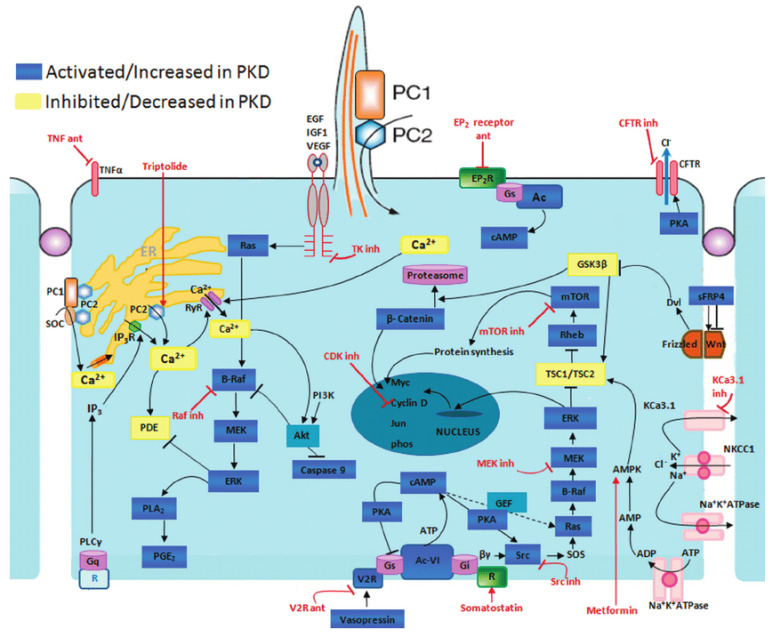
Autosomal dominant polycystic kidney disease (ADPKD) is the most common genetic renal disease, with an estimated prevalence between 1:1000 and 1:2500. It is mostly caused by mutations of the PKD1 and PKD2 genes encoding polycystin 1 (PC1) and polycystin 2 (PC2) that regulate cellular processes such as fluid transport, differentiation, proliferation, apoptosis and cell adhesion. Reduction of calcium ions and induction of cyclic adenosine monophosphate (sAMP) promote cyst enlargement by transepithelial fluid secretion and cell proliferation. Abnormal activation of MAPK/ERK pathway, dysregulated signaling of heterotrimeric G proteins, mTOR, phosphoinositide 3-kinase, AMPK, JAK/STAT activator of transcription and nuclear factor kB (NF-kB) are involved in cystogenesis. Another feature of cystic tissue is increased extracellular production and recruitment of inflammatory cells and abnormal connections among cells. Moreover, metabolic alterations in cystic cells including defective glucose metabolism, impaired beta-oxidation and abnormal mitochondrial activity were shown to be associated with cyst expansion. Although tolvaptan has been recently approved as a drug that slows ADPKD progression, some patients do not tolerate tolvaptan because of frequent aquaretic. The advances in the knowledge of multiple molecular pathways involved in cystogenesis led to the development of animal and cellular studies, followed by the development of several ongoing randomized controlled trials with promising drugs. Our review is aimed at pathophysiological mechanisms in cystogenesis in connection with the most promising drugs in animal and clinical studies.
Keywords: autosomal dominant polycystic kidney disease; cystogenesis; therapy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Neumann H.P., Jilg C., Bacher J., Nabulsi Z., Malinoc A., Hummel B., Hoffmann M.M., Ortiz-Bruechle N., Glasker S., Pisarski P. Epidemiology of autosomal-dominant polycystic kidney disease: An in-depth clinical study for south-western Germany. Nephrol. Dial. Transplant. 2013;28:1472–1487. doi: 10.1093/ndt/gfs551. - DOI - PubMed
-
- Spithoven E.M., Kramer A., Meijer E., Orskov B., Wanner C., Abad J.M., Aresté N., De La Torre R.A., Caskey F., Couchoud C., et al. Renal replacement therapy for autosomal dominant polycystic kidney disease (ADPKD) in Europe: Prevalence and survival—An analysis of data from the ERA-EDTA Registry. Nephrol. Dial. Transplant. 2014;29:iv15–iv25. doi: 10.1093/ndt/gfu017. - DOI - PMC - PubMed
-
- Chapman A.B., Guay-Woodford L.M., Grantham J.J., Torres V.E., Bae K.T., Baumgarten D.A., Kenney P.J., King B.F., Glockner J.F., Wetzel L.H., et al. Renal structure in early autosomal-dominant polycystic kidney disease (ADPKD): The Consortium for Radiologic Imaging Studies of Polycystic Kidney Disease (CRISP) cohort1. Kidney Int. 2003;64:1035–1045. doi: 10.1046/j.1523-1755.2003.00185.x. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
