

Coagulopathy and Fibrinolytic Pathophysiology in COVID-19 and SARS-CoV-2 Vaccination
- PMID: 35328761
- PMCID: PMC8955234
- DOI: 10.3390/ijms23063338
Coagulopathy and Fibrinolytic Pathophysiology in COVID-19 and SARS-CoV-2 Vaccination
Abstract
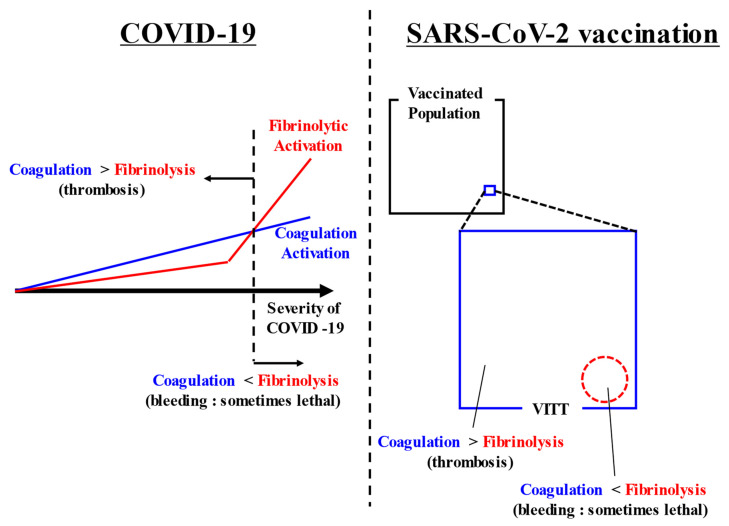
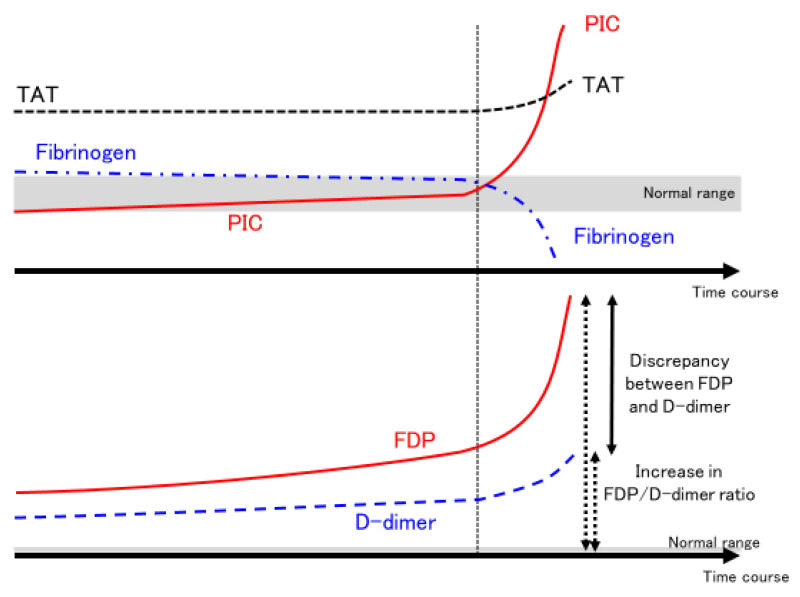
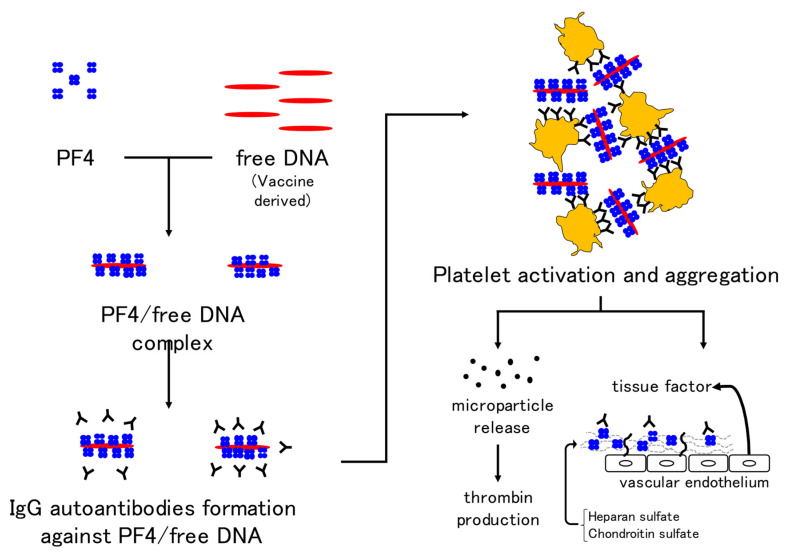
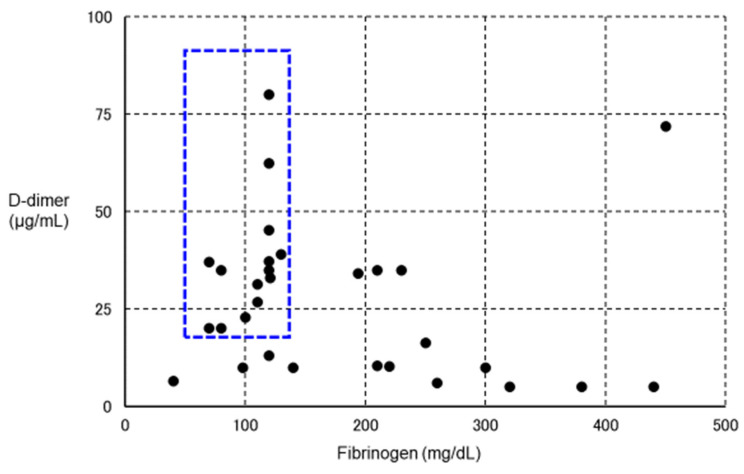
Coronavirus Disease 2019 (COVID-19) is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and is frequently complicated by thrombosis. In some cases of severe COVID-19, fibrinolysis may be markedly enhanced within a few days, resulting in fatal bleeding. In the treatment of COVID-19, attention should be paid to both coagulation activation and fibrinolytic activation. Various thromboses are known to occur after vaccination with SARS-CoV-2 vaccines. Vaccine-induced immune thrombotic thrombocytopenia (VITT) can occur after adenovirus-vectored vaccination, and is characterized by the detection of anti-platelet factor 4 antibodies by enzyme-linked immunosorbent assay and thrombosis in unusual locations such as cerebral venous sinuses and visceral veins. Treatment comprises high-dose immunoglobulin, argatroban, and fondaparinux. Some VITT cases show marked decreases in fibrinogen and platelets and marked increases in D-dimer, suggesting the presence of enhanced-fibrinolytic-type disseminated intravascular coagulation with a high risk of bleeding. In the treatment of VITT, evaluation of both coagulation activation and fibrinolytic activation is important, adjusting treatments accordingly to improve outcomes.
Keywords: COVID-19; SARS-CoV-2 vaccine; coagulopathy; enhanced-fibrinolytic-type DIC; fibrinolysis; nafamostat.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
