

Unreliability of Clinical Prediction Rules to Exclude without Echocardiography Infective Endocarditis in Staphylococcus aureus Bacteremia
- PMID: 35329827
- PMCID: PMC8955153
- DOI: 10.3390/jcm11061502
Unreliability of Clinical Prediction Rules to Exclude without Echocardiography Infective Endocarditis in Staphylococcus aureus Bacteremia
Abstract
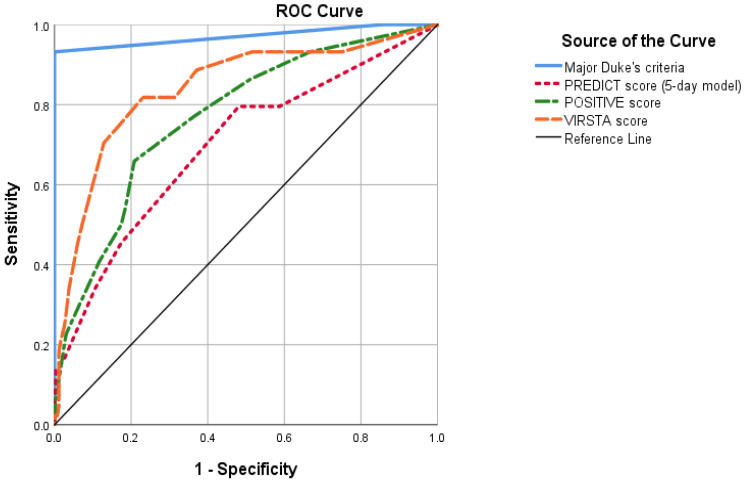
Background: It is unclear whether the use of clinical prediction rules is sufficient to rule out infective endocarditis (IE) in patients with Staphylococcus aureus bacteremia (SAB) without an echocardiogram evaluation, either transthoracic (TTE) and/or transesophageal (TEE). Our primary purpose was to test the usefulness of PREDICT, POSITIVE, and VIRSTA scores to rule out IE without echocardiography. Our secondary purpose was to evaluate whether not performing an echocardiogram evaluation is associated with higher mortality.
Methods: We conducted a unicentric retrospective cohort including all patients with a first SAB episode from January 2015 to December 2020. IE was defined according to modified Duke criteria. We predefined threshold cutoff points to consider that IE was ruled out by means of the mentioned scores. To assess 30-day mortality, we used a multivariable regression model considering performing an echocardiogram as covariate.
Results: Out of 404 patients, IE was diagnosed in 50 (12.4%). Prevalence of IE within patients with negative PREDICT, POSITIVE, and VIRSTA scores was: 3.6% (95% CI 0.1-6.9%), 4.9% (95% CI 2.2-7.7%), and 2.2% (95% CI 0.2-4.3%), respectively. Patients with negative VIRSTA and negative TTE had an IE prevalence of 0.9% (95% CI 0-2.8%). Performing an echocardiogram was independently associated with lower 30-day mortality (OR 0.24 95% CI 0.10-0.54, p = 0.001).
Conclusion: PREDICT and POSITIVE scores were not sufficient to rule out IE without TEE. In patients with negative VIRSTA score, it was doubtful if IE could be discarded with a negative TTE. Not performing an echocardiogram was associated with worse outcomes, which might be related to presence of occult IE. Further studies are needed to assess the usefulness of clinical prediction rules in avoiding echocardiographic evaluation in SAB patients.
Keywords: Staphylococcus aureus; clinical prediction rules; echocardiography; endocarditis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Validation of VIRSTA and Predicting Risk of Endocarditis Using a Clinical Tool (PREDICT) Scores to Determine the Priority of Echocardiography in Patients With Staphylococcus aureus Bacteremia.Clin Infect Dis. 2021 Sep 7;73(5):e1151-e1157. doi: 10.1093/cid/ciaa1844. Clin Infect Dis. 2021. PMID: 34492692
-
Use of Transthoracic Echocardiography in the Management of Low-Risk Staphylococcus aureus Bacteremia: Results From a Retrospective Multicenter Cohort Study.JACC Cardiovasc Imaging. 2015 Aug;8(8):924-31. doi: 10.1016/j.jcmg.2015.02.027. Epub 2015 Jul 15. JACC Cardiovasc Imaging. 2015. PMID: 26189120
-
Prediction Rules for Ruling Out Endocarditis in Patients With Staphylococcus aureus Bacteremia.Clin Infect Dis. 2022 Apr 28;74(8):1442-1449. doi: 10.1093/cid/ciab632. Clin Infect Dis. 2022. PMID: 34272564 Free PMC article.
-
Clinical Risk Factors for Infective Endocarditis Patients With Staphylococcus Aureus Bacteremia and the Diagnostic Utility of Transesophageal Echocardiogram.Curr Probl Cardiol. 2022 Nov;47(11):101331. doi: 10.1016/j.cpcardiol.2022.101331. Epub 2022 Jul 20. Curr Probl Cardiol. 2022. PMID: 35870547 Review.
-
Appropriate use of echocardiography in managing Staphylococcus aureus bacteremia.Expert Rev Anti Infect Ther. 2012 Apr;10(4):501-8. doi: 10.1586/eri.12.22. Expert Rev Anti Infect Ther. 2012. PMID: 22512758 Review.
Cited by
-
The Changing Complementary Role of Multimodality Imaging in Clinical Cardiology.J Clin Med. 2022 Nov 30;11(23):7095. doi: 10.3390/jcm11237095. J Clin Med. 2022. PMID: 36498670 Free PMC article.
-
The LAUsanne STAPHylococcus aureus ENdocarditis (LAUSTAPHEN) score: A prediction score to estimate initial risk for infective endocarditis in patients with S. aureus bacteremia.Front Cardiovasc Med. 2022 Dec 9;9:961579. doi: 10.3389/fcvm.2022.961579. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36568565 Free PMC article.
-
Unexpected Infective Endocarditis: Towards a New Alert for Clinicians.J Clin Med. 2024 Aug 26;13(17):5058. doi: 10.3390/jcm13175058. J Clin Med. 2024. PMID: 39274271 Free PMC article. Review.
-
Risk of endocarditis among patients with coagulase-negative Staphylococcus bacteremia.Sci Rep. 2023 Sep 20;13(1):15613. doi: 10.1038/s41598-023-41888-7. Sci Rep. 2023. PMID: 37730691 Free PMC article.
References
-
- Kuehl R., Morata L., Boeing C., Subirana I., Seifert H., Rieg S., Kern W.V., Kim H.B., Kim E.S., Liao C.H., et al. Defining persistent Staphylococcus aureus bacteraemia: Secondary analysis of a prospective cohort study. Lancet Infect. Dis. 2020;20:1409–1417. doi: 10.1016/S1473-3099(20)30447-3. - DOI - PubMed
-
- Hidalgo-Tenorio C., Gálvez J., Martínez-Marcos F.J., Plata-Ciezar A., De La Torre-Lima J., López-Cortés L.E., Noureddine M., Reguera J.M., Vinuesa D., García M.V., et al. Clinical and prognostic differences between methicillin-resistant and methicillin-susceptible Staphylococcus aureus infective endocarditis. BMC Infect. Dis. 2020;20:160. doi: 10.1186/s12879-020-4895-1. - DOI - PMC - PubMed
-
- Hsu R.-B. Risk Factors for Nosocomial Infective Endocarditis in Patients with Methicillin-Resistant Staphylococcus Aureus Bacteremia. [(accessed on 13 October 2021)];Infect. Control Hosp. Epidemiol. 2005 26:654–657. doi: 10.1086/502597. Available online: https://www.cambridge.org/core/product/identifier/S0899823X00198605/type.... - DOI - PubMed
-
- Mensa J., Soriano A., Llinares P., Barberán J., Montejo M., Salavert M., Alvarez-Rocha L., Maseda E., Moreno A., Pasquau J., et al. Guía de tratamiento antimicrobiano de la infección por Staphylococcus aureus. Rev. Esp. Quim. Publ. Soc. Esp. Quim. 2013;26((Suppl. 1)):1–84. - PubMed
LinkOut - more resources
Full Text Sources
