

Conditions for Achieving Postoperative Pelvic Incidence-Lumbar Lordosis < 10° in Circumferential Minimally Invasive Surgery for Adult Spinal Deformity
- PMID: 35329912
- PMCID: PMC8951564
- DOI: 10.3390/jcm11061586
Conditions for Achieving Postoperative Pelvic Incidence-Lumbar Lordosis < 10° in Circumferential Minimally Invasive Surgery for Adult Spinal Deformity
Abstract
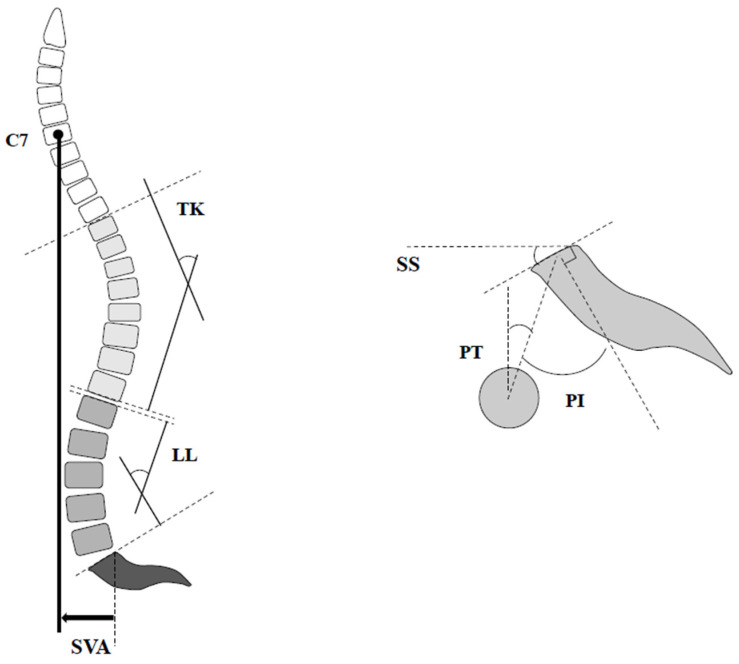
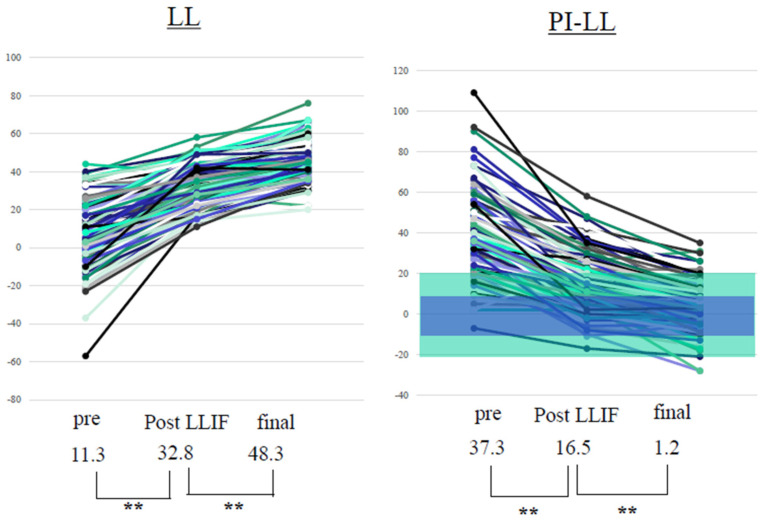
This retrospective study aimed to evaluate the clinical outcomes of circumferential minimally invasive surgery (CMIS) using lateral lumbar interbody fusion (LLIF) and percutaneous pedicle screw (PPS) in adult spinal deformity (ASD) patients, and to clarify the conditions for achieving postoperative pelvic incidence-lumbar lordosis (PI-LL) < 10°. Demographics and other parameters of ASD patients who underwent CMIS and who were divided into groups G (achieved postoperative PI-LL < 10°) and P (PI-LL ≥ 10°) were compared. Of the 145 included ASD patients who underwent CMIS, the average fused level, bleeding volume, operative time, and number of intervertebral discs that underwent LLIF were 10.3 ± 0.5 segments, 723 ± 375 mL, 366 ± 70 min, and 4.0 segments, respectively. The rod material was titanium alloy in all the cases. The PI-LL significantly improved from 37.3 ± 17.9° to 1.2 ± 12.2° postoperatively. Pre- and postoperative PI, postoperative LL, preoperative PI-LL, PI-LL after LLIF, and postoperative PI-LL were significantly larger in group P. PI-LL after LLIF was identified as a significant risk factor of postoperative PI-LL < 10° by logistic regression, and the cut-off value on receiver operating characteristic curve analysis was 20°. Sufficient correction was achieved by CMIS. If PI-LL after LLIF was ≤20°, it was corrected to the ideal alignment by the PPS procedure.
Keywords: adult spinal deformity; circumferential minimally invasive surgery; lateral lumbar interbody fusion; lumbosacral fusion; percutaneous pedicle screw.
Conflict of interest statement
All authors declared that there are no conflict of interest.
Figures


Similar articles
-
Comparison of two minimally invasive surgery strategies to treat adult spinal deformity.J Neurosurg Spine. 2015 Apr;22(4):374-80. doi: 10.3171/2014.9.SPINE131004. Epub 2015 Jan 30. J Neurosurg Spine. 2015. PMID: 25635632
-
Correction of severe spinopelvic mismatch: decreased blood loss with lateral hyperlordotic interbody grafts as compared with pedicle subtraction osteotomy.Neurosurg Focus. 2017 Aug;43(2):E15. doi: 10.3171/2017.5.FOCUS17195. Neurosurg Focus. 2017. PMID: 28760028
-
Does approach matter? A comparative radiographic analysis of spinopelvic parameters in single-level lumbar fusion.Spine J. 2018 Nov;18(11):1999-2008. doi: 10.1016/j.spinee.2018.03.014. Epub 2018 Apr 6. Spine J. 2018. PMID: 29631061
-
Clinical and radiographic parameters associated with best versus worst clinical outcomes in minimally invasive spinal deformity surgery.J Neurosurg Spine. 2016 Jul;25(1):21-5. doi: 10.3171/2015.12.SPINE15999. Epub 2016 Mar 4. J Neurosurg Spine. 2016. PMID: 26943254
-
Restoration of lumbar lordosis after minimally invasive transforaminal lumbar interbody fusion: a systematic review.Spine J. 2019 May;19(5):951-958. doi: 10.1016/j.spinee.2018.10.017. Epub 2018 Dec 6. Spine J. 2019. PMID: 30529420
Cited by
-
Bone Fusion Morphology after Circumferential Minimally Invasive Spine Surgery Using Lateral Lumbar Interbody Fusion and Percutaneous Pedicle Screws without Bone Grafting in the Thoracic Spine: A Retrospective Study.Medicina (Kaunas). 2022 Mar 30;58(4):496. doi: 10.3390/medicina58040496. Medicina (Kaunas). 2022. PMID: 35454335 Free PMC article.
-
Simplified S1 vertebral bone quality score independently predicts proximal junctional kyphosis after surgery for degenerative lumbar scoliosis.J Orthop Surg Res. 2024 Apr 13;19(1):238. doi: 10.1186/s13018-024-04722-y. J Orthop Surg Res. 2024. PMID: 38615068 Free PMC article. Review.
-
New Effective Intraoperative Techniques for the Prevention of Coronal Imbalance after Circumferential Minimally Invasive Correction Surgery for Adult Spinal Deformity.J Clin Med. 2023 Aug 31;12(17):5670. doi: 10.3390/jcm12175670. J Clin Med. 2023. PMID: 37685737 Free PMC article.
References
-
- Bess S., Line B., Fu K.M., McCarthy I., Lafage V., Schwab F., Shaffrey C., Ames C., Akbarnia B., Jo H., et al. The health impact of symptomatic adult spinal deformity: Comparison of deformity types to United States population norms and chronic diseases. Spine. 2016;41:224–233. doi: 10.1097/BRS.0000000000001202. - DOI - PMC - PubMed
-
- Acaroglu E., Yavuz A.C., Guler U.O., Yuksel S., Yavuz Y., Domingo-Sabat M., Pellise F., Alanay A., Perez Grueso F.S., Kleinstück F., et al. A decision analysis to identify the ideal treatment for adult spinal deformity: Is surgery better than non-surgical treatment in improving health-related quality of life and decreasing the disease burden? Eur. Spine J. 2016;25:2390–2400. doi: 10.1007/s00586-016-4413-8. - DOI - PubMed
-
- Gum J.L., Glassman S.D., Douglas L.R., Carreon L.Y. Correlation between cervical spine sagittal alignment and clinical outcome after anterior cervical discectomy and fusion. Am. J. Orthop. 2012;41:E81–E84. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
