

Echocardiography Nomogram for Predicting Survival among Chronic Lung Disease Patients with Severe Pulmonary Hypertension
- PMID: 35329931
- PMCID: PMC8955171
- DOI: 10.3390/jcm11061603
Echocardiography Nomogram for Predicting Survival among Chronic Lung Disease Patients with Severe Pulmonary Hypertension
Abstract
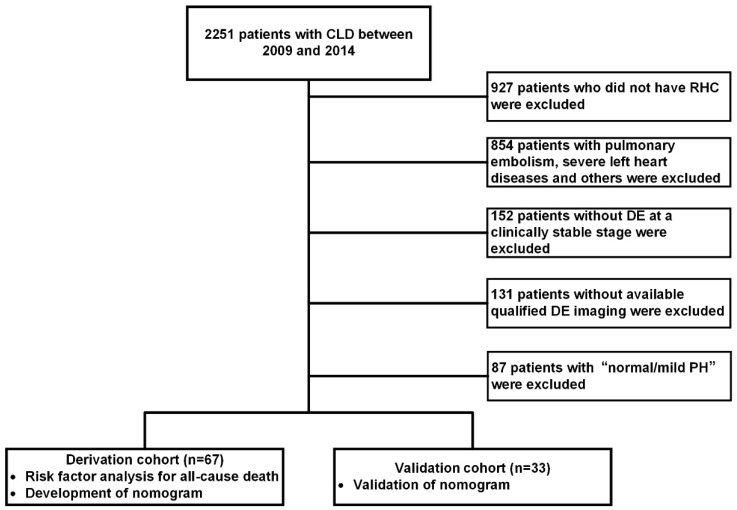
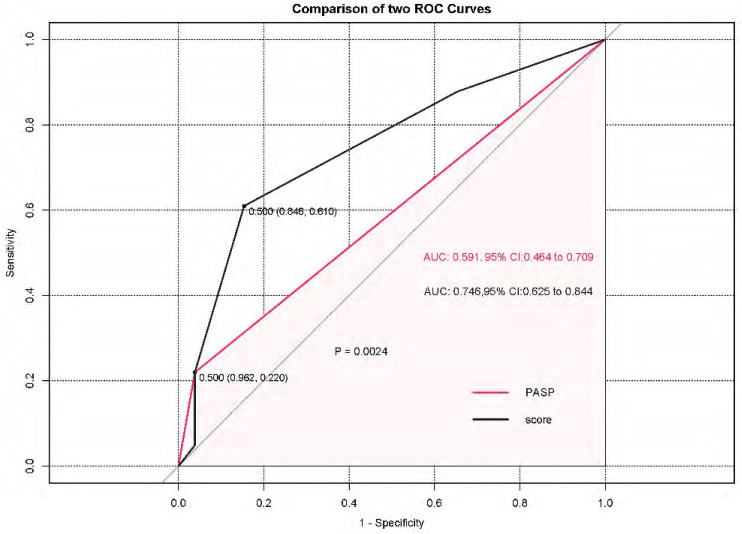
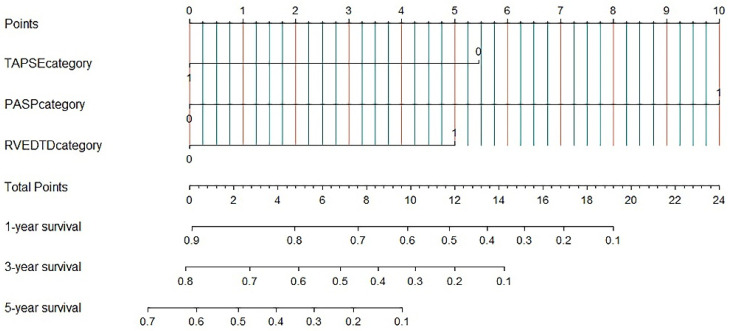
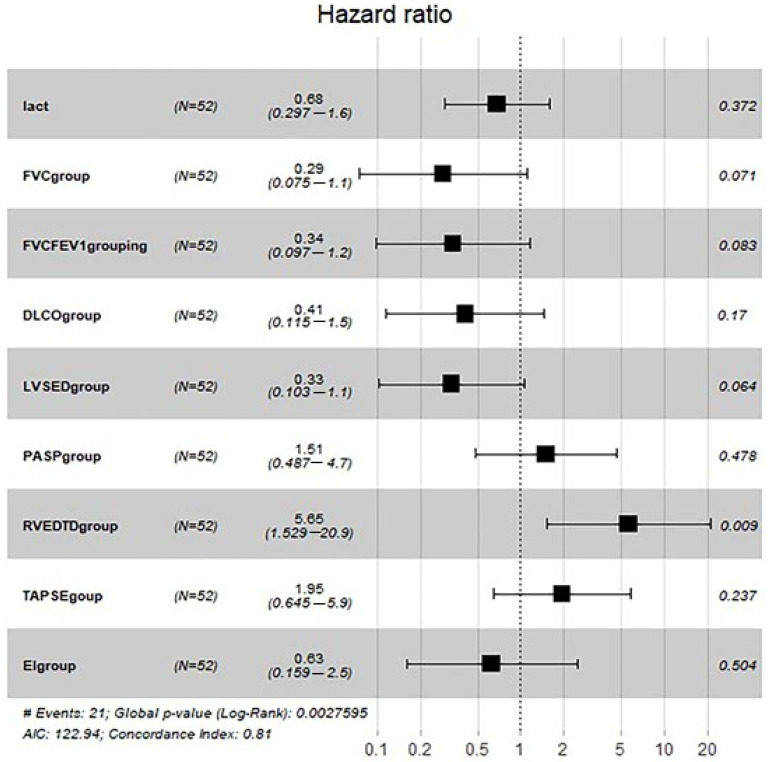
Severe pulmonary hypertension in chronic lung diseases (severe CLD-PH) differs significantly from other types of PH in physiology and prognosis. We aimed to assess whether echocardiography helps predict long-term survival in patients with severe CLD-PH. This single-centre, observational cohort study enrolled 100 patients with severe CLD-PH (mean pulmonary arterial pressure ≥35 mm Hg or ≥25 mm Hg with cardiac index <2.0 L/min/m2 or pulmonary vascular resistance ≥6 Wood units) between 2009 and 2014. The population was randomly divided into a derivation and validation cohort in a 2:1 ratio. To construct a nomogram, a multivariable logistic regression model was applied, and scores were assigned based on the hazard ratio of independent echocardiographic predictors. Multivariate Cox hazards analysis identified the strongest predictors of mortality as pulmonary arterial systolic pressure (PASP), tricuspid annular plane systolic excursion, and right ventricular end-diastolic transverse dimension. The three independent predictors were entered into the nomogram. Compared with PASP alone, the nomogram resulted in an integrated discrimination improvement of 15.5% (95% confidence interval, 5.52−25.5%, p = 0.002) with a net improvement in model discrimination (C-statistic from 0.591 to 0.746). Using echocardiographic parameters, we established and validated a novel nomogram to predict all-cause death for patients with severe CLD-PH.
Keywords: chronic lung diseases; echocardiography; haemodynamics; pulmonary hypertension; right heart catheterization; survival.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Simonneau G., Gatzoulis M.A., Adatia I., Celermajer D., Denton C., Ghofrani A., Sanchez M.A.G., Kumar R.K., Landzberg M., Machado R.F., et al. Updated clinical classification of pulmonary hypertension. J. Am. Coll. Cardiol. 2013;62((Suppl. 25)):D34–D41. doi: 10.1016/j.jacc.2013.10.029. - DOI - PubMed
-
- Hoeper M.M., Andreas S., Bastian A., Claussen M., Ghofrani H.A., Gorenflo M., Grohé C., Günther A., Halank M., Hammerl P., et al. Pulmonary hypertension due to chronic lung disease: Updated Recommendations of the Cologne Consensus Conference 2011. Int. J. Cardiol. 2011;154((Suppl. 1)):S45–S53. doi: 10.1016/S0167-5273(11)70492-2. - DOI - PubMed
-
- Kovacs G., Agusti A., Barbera J.A., Celli B., Criner G., Humbert M., Sin D.D., Voelkel N., Olschewski H. Pulmonary Vascular Involvement in Chronic Obstructive Pulmonary Disease. Is There a Pulmonary Vascular Phenotype? Am. J. Respir. Crit. Care Med. 2018;198:1000–1011. doi: 10.1164/rccm.201801-0095PP. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
