

Different Methods to Improve the Monitoring of Noninvasive Respiratory Support of Patients with Severe Pneumonia/ARDS Due to COVID-19: An Update
- PMID: 35330029
- PMCID: PMC8952765
- DOI: 10.3390/jcm11061704
Different Methods to Improve the Monitoring of Noninvasive Respiratory Support of Patients with Severe Pneumonia/ARDS Due to COVID-19: An Update
Abstract
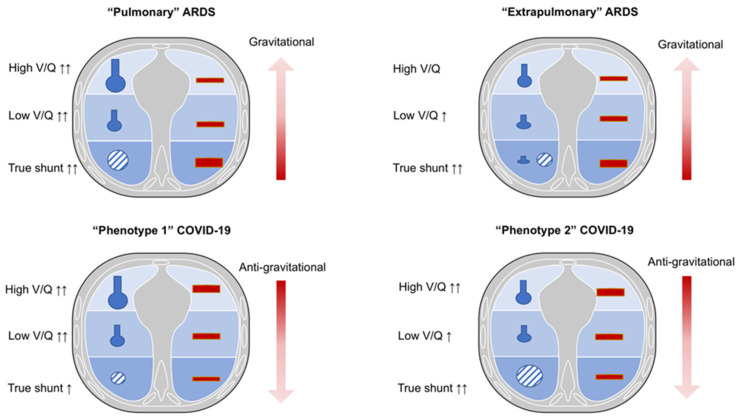
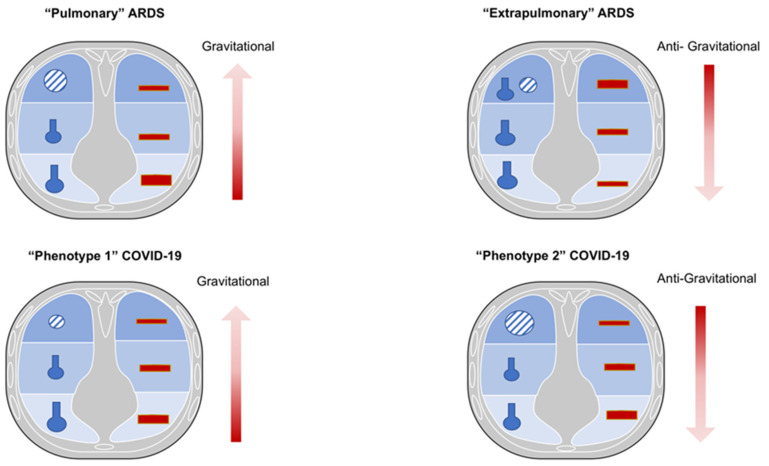
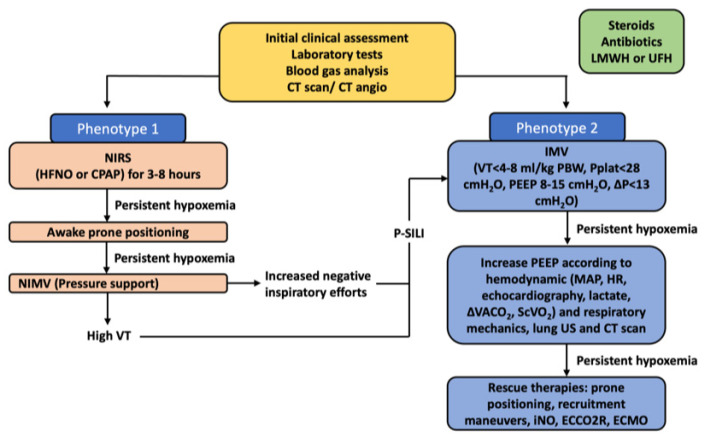
The latest guidelines for the hospital care of patients affected by coronavirus disease 2019 (COVID-19)-related acute respiratory failure have moved towards the widely accepted use of noninvasive respiratory support (NIRS) as opposed to early intubation at the pandemic onset. The establishment of severe COVID-19 pneumonia goes through different pathophysiological phases that partially resemble typical acute respiratory distress syndrome (ARDS) and have been categorized into different clinical-radiological phenotypes. These can variably benefit on the application of external positive end-expiratory pressure (PEEP) during noninvasive mechanical ventilation, mainly due to variable levels of lung recruitment ability and lung compliance during different phases of the disease. A growing body of evidence suggests that intense respiratory effort producing excessive negative pleural pressure swings (Ppl) plays a critical role in the onset and progression of lung and diaphragm damage in patients treated with noninvasive respiratory support. Routine respiratory monitoring is mandatory to avoid the nasty continuation of NIRS in patients who are at higher risk for respiratory deterioration and could benefit from early initiation of invasive mechanical ventilation instead. Here we propose different monitoring methods both in the clinical and experimental settings adapted for this purpose, although further research is required to allow their extensive application in clinical practice. We reviewed the needs and available tools for clinical-physiological monitoring that aims at optimizing the ventilatory management of patients affected by acute respiratory distress syndrome due to severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) infection.
Keywords: ARDS; COVID-19; coronavirus disease; noninvasive respiratory support (NIRS); respiratory failure.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- WHO WHO Coronavirus (COVID-19) Dashboard. 2021. [(accessed on 16 February 2022)]. Available online: https://covid19.who.int.
-
- Hermann M., Laxar D., Krall C., Hafner C., Herzog O., Kimberger O. Duration of invasive mechanical ventilation prior to extracorporeal membrane oxygenation is not associated with survival in acute respiratory distress syndrome caused by coronavirus disease 2019. Ann. Intensive Care. 2022;12:6. doi: 10.1186/s13613-022-00980-3. - DOI - PMC - PubMed
-
- Ball L., Barisione E., Mastracci L., Campora M., Costa D., Robba C., Battaglini D., Micali M., Costantino F., Cittadini G., et al. Extension of Collagen Deposition in COVID-19 Post Mortem Lung Samples and Computed Tomography Analysis Findings. Int. J. Mol. Sci. 2021;22:7498. doi: 10.3390/ijms22147498. - DOI - PMC - PubMed
-
- Baratella E., Ruaro B., Marrocchio C., Starvaggi N., Salton F., Giudici F., Quaia E., Confalonieri M., Cova M.A. Interstitial Lung Disease at High Resolution CT after SARS-CoV-2-Related Acute Respiratory Distress Syndrome According to Pulmonary Segmental Anatomy. J. Clin. Med. 2021;10:3985. doi: 10.3390/jcm10173985. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
