

Reducing Tolerance for SABA and OCS towards the Extreme Ends of Asthma Severity
- PMID: 35330503
- PMCID: PMC8949541
- DOI: 10.3390/jpm12030504
Reducing Tolerance for SABA and OCS towards the Extreme Ends of Asthma Severity
Abstract
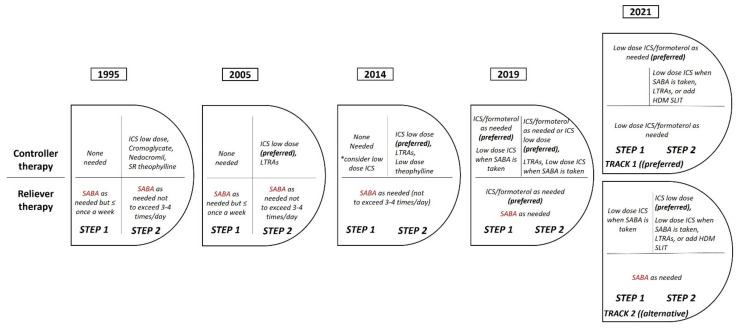
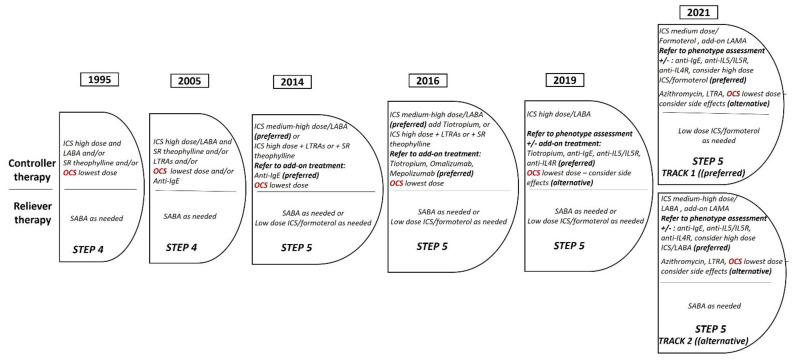
Asthma is a heterogeneous chronic inflammatory airway disease that imposes a great burden on public health worldwide. In the past two years, fundamental changes have been addressed in the Global Initiative for Asthma (GINA) recommendations focusing mainly on the management of mild and severe asthma. The use of as-needed treatment containing inhaled corticosteroids plus fast-acting bronchodilators (either short or long-acting formoterol) in mild asthma has dominated the field, and both randomized and real-world studies favor such an approach and associate it with fewer exacerbations and good asthma control. At the same time, the effort to diminish the use of oral steroids (OCS) as maintenance treatment in severe asthma was substantially accomplished with the initiation of treatment with biologics. Still, these options are available at the moment only for severe asthmatics with a T2-high endotype, and relevant studies on biologics have yielded, as a primary outcome, the reduction or even cessation of OCS. Accordingly, OCS should be considered as a temporary option, mainly for the treatment of asthma exacerbations, and as a maintenance treatment only for a minority of patients with severe asthma, after ensuring good inhaler technique, modification of all possible contributory factors and comorbidities, and optimized pharmacotherapy using all other add-on treatments including biologics in the armamentarium of anti-asthma medication.
Keywords: asthma; mild asthma; oral corticosteroids; severe asthma; short-acting beta-agonists.
Conflict of interest statement
PB has received honoraria for presentations and consultancy fees from AstraZeneca, Boehringer Ingelheim, Chiesi, ELPEN, GSK, Menarini, Novartis, Sanofi, and Gilead. KK: has received honoraria for presentations and consultancy fees from AstraZeneca, Boehringer Ingelheim, CSL Behring, Chiesi, ELPEN, GSK, Menarini, Novartis and Sanofi (paid to the University of Ioannina). His department has received funding and grants from AstraZeneca, Boehringer Ingelheim, Chiesi, Innovis, ELPEN, GSK, Menarini, Novartis and NuvoAir (paid to the University of Ioannina). SL: has received honoraria for presentations and consultancy fees from AstraZeneca, Boehringer Ingelheim, Chiesi, ELPEN, GSK, Sanofi, Pfizer, Menarini, MSD, Gilead. MM: has received honoraria for presentations and consultancy fees from AstraZeneca, Chiesi, Novartis, GSK, Sanofi, Pfizer, Menarini. NGP: Speaker, advisor at ALK, Asit Biotech, AstraZeneca, Biomay, Boehringer Ingelheim, GSK, HAL, Faes Farma, Medscape, Menarini, MSD, Mylan/Meda, Novartis, Nutricia, OM Pharma, Regeneron, Sanofi, Takeda. PS: has received honoraria for presentations and consultancy fees from AstraZeneca, Boehringer Ingelheim, Chiesi, ELPEN, GSK, and Menarini (paid to the Democritus University of Thrace). His department has received funding and grants from AstraZeneca, Boehringer Ingelheim, Chiesi, ELPEN, GSK, and Menarini (paid to the Democritus University of Thrace). ST: has received honoraria for presentations and consultancy fees from AstraZeneca, Boehringer Ingelheim, ELPEN, Menarini. His department has received grants from AstraZeneca, Chiesi, ELPEN, GSK. EZ: has received honoraria for presentations and consultancy fees from AstraZeneca, Boehringer Ingelheim, Chiesi, ELPEN, GSK, Menarini, Novartis and Sanofi.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
