

Total Hip Arthroplasty in Patients With Severe Chronic Pubic Diastasis
- PMID: 35330667
- PMCID: PMC8938874
- DOI: 10.1016/j.artd.2022.02.017
Total Hip Arthroplasty in Patients With Severe Chronic Pubic Diastasis
Abstract
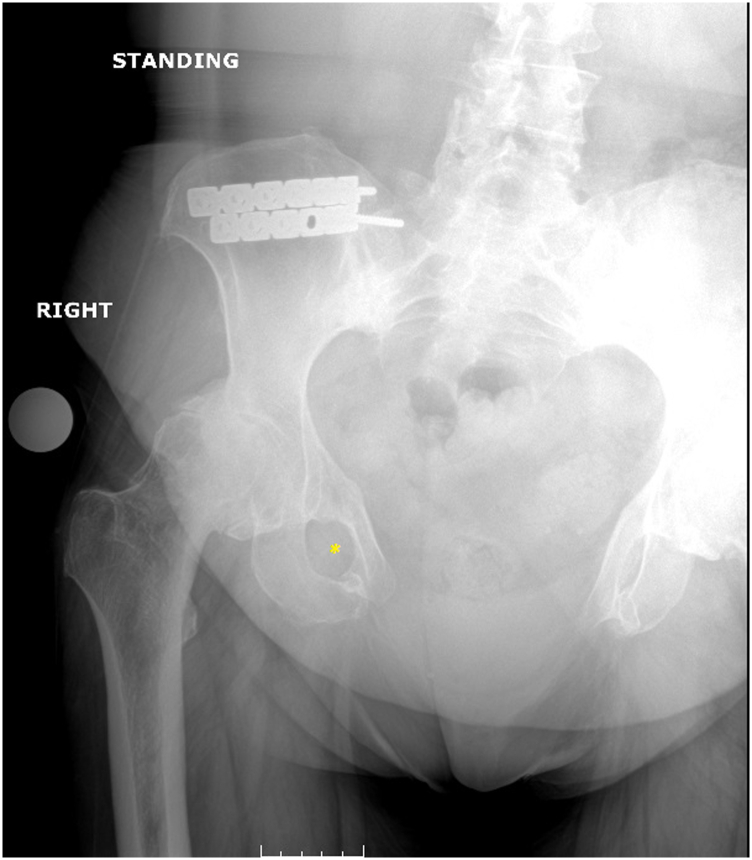
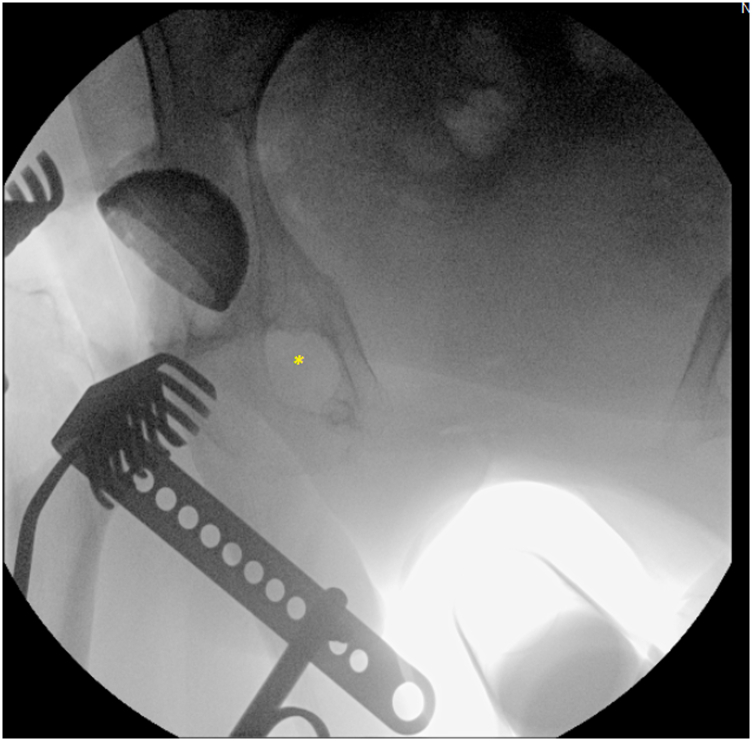
Background: Total hip arthroplasty (THA) in patients with severe chronic pubic diastasis from either congenital or acquired causes presents an exceptionally difficult challenge that has rarely been addressed in the arthroplasty literature. The purpose of this paper is to present a series of THAs in patients with severe chronic pubic diastasis, asking the following research questions: (1) What is the survivorship and clinical outcomes after THA in patients with severe chronic pubic diastasis? And (2) What is the rate of complications after THA surgery in this challenging patient population? We additionally describe our algorithm for preoperative planning and rationale for surgical technique and implant position.
Material and methods: We retrospectively queried the prospective arthroplasty database of 2 high-volume referral centers, yielding 6 THA in 4 patients with severe chronic pubic diastasis (minimum 8 cm) with a mean follow-up of 2.7 years. We recorded baseline demographic and intraoperative variables, as well as survivorship, patient-reported outcomes (Hip disability and Osteoarthritis Outcome Score for Joint Replacement score), and incidence of complications.
Results: There were no failures reported (100% survivorship) at a mean follow-up of 2.7 years. Mean Hip disability and Osteoarthritis Outcome Score for Joint Replacement scores improved from 36.0 preoperatively to 82.8 postoperatively. There were no infections, dislocations, fractures, or any major complications in the postoperative period.
Conclusion: THA for patients with severe chronic pubic diastasis remains a rare but challenging reconstructive procedure. Excellent outcomes can be achieved with adequate preparation, particularly regarding the acetabular component position. Understanding the nature of the hemipelvis deformity and meticulous templating using "normalized" views of the hip are important components to a successful preoperative plan.
Keywords: Patient-reported outcomes; Pre-operative planning; Pubic diastasis; Survivorship; Total hip arthroplasty.
© 2022 The Authors.
Figures



References
-
- Learmonth I.D., Young C., Rorabeck C. The operation of the century: total hip replacement. Lancet. 2007;370:1508. - PubMed
-
- Greber E.M., Pelt C.E., Gililland J.M., Anderson M.B., Erickson J.A., Peters C.L. Challenges in total hip arthroplasty in the setting of developmental dysplasia of the hip. J Arthroplasty. 2017;32(9S):S38. - PubMed
-
- Dapuzzo M.R., Sierra R.J. Acetabular considerations during total hip arthroplasty for hip dysplasia. Orthop Clin North Am. 2012;43(3):369. - PubMed
-
- Hanna S.A., Sarraf K.M., Ramachandran M., Achan P. Systematic review of the outcome of total hip arthroplasty in patients with sequelae of Legg-Calve-Perthes disease. Arch Orthop Trauma Surg. 2017;137(8):1149. - PubMed
LinkOut - more resources
Full Text Sources
