

A Loading Dose of Dexmedetomidine With Constant Infusion Inhibits Intraoperative Neuromonitoring During Thoracic Spinal Decompression Surgery: A Randomized Prospective Study
- PMID: 35330828
- PMCID: PMC8940210
- DOI: 10.3389/fphar.2022.840320
A Loading Dose of Dexmedetomidine With Constant Infusion Inhibits Intraoperative Neuromonitoring During Thoracic Spinal Decompression Surgery: A Randomized Prospective Study
Abstract
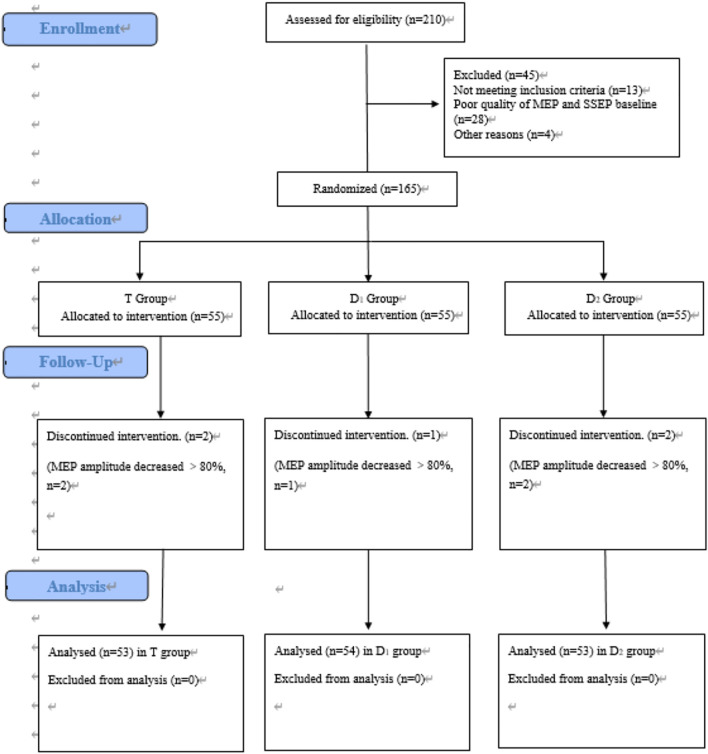
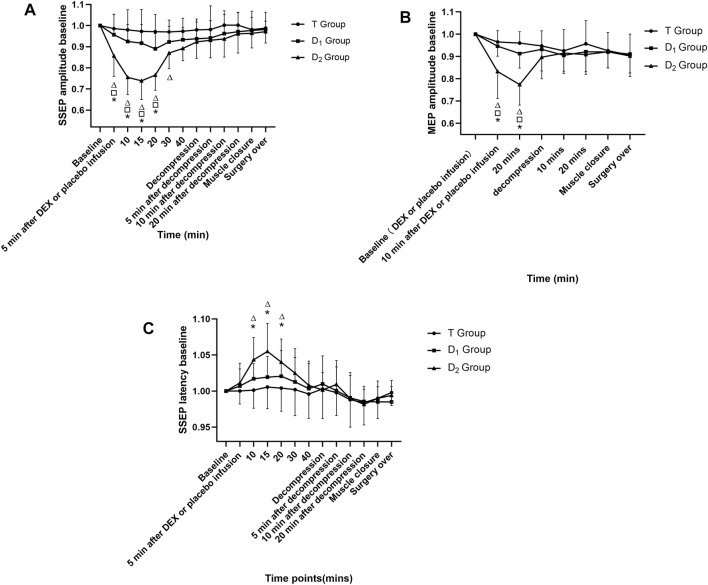
Background: The effect of a bolus dose of dexmedetomidine on intraoperative neuromonitoring (IONM) parameters during spinal surgeries has been variably reported and remains a debated topic. Methods: A randomized, double-blinded, placebo-controlled study was performed to assess the effect of dexmedetomidine (1 μg/kg in 10 min) followed by a constant infusion rate on IONM during thoracic spinal decompression surgery (TSDS). A total of 165 patients were enrolled and randomized into three groups. One group received propofol- and remifentanil-based total intravenous anesthesia (TIVA) (T group), one group received TIVA combined with dexmedetomidine at a constant infusion rate (0.5 μg kg-1 h-1) (D1 group), and one group received TIVA combined with dexmedetomidine delivered in a loading dose (1 μg kg-1 in 10 min) followed by a constant infusion rate (0.5 μg kg-1 h-1) (D2 group). The IONM data recorded before test drug administration was defined as the baseline value. We aimed at comparing the parameters of IONM. Results: In the D2 group, within-group analysis showed suppressive effects on IONM parameters compared with baseline value after a bolus dose of dexmedetomidine. Furthermore, the D2 group also showed inhibitory effects on IONM recordings compared with both the D1 group and the T group, including a statistically significant decrease in SSEP amplitude and MEP amplitude, and an increase in SSEP latency. No significance was found in IONM parameters between the T group and the D1 group. Conclusion: Dexmedetomidine delivered in a loading dose can significantly inhibit IONM parameters in TSDS. Special attention should be paid to the timing of a bolus dose of dexmedetomidine under IONM. However, dexmedetomidine delivered at a constant speed does not exert inhibitory effects on IONM data.
Keywords: dexmedetomidine; intraoperative neuromonitoring; motor evoked potential (MEP); somatosensory evoked potential (SSEP); thoracic spinal decompression surgery.
Copyright © 2022 Liu, Qin, Qi, Luo, Yan, Yu, Dong, Zhao, Wu, Chang, Liu, Liu, Yuan, Li, Xiao and Wang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Variability of somatosensory evoked potential and motor evoked potential change criteria in thoracic spinal decompression surgery based on preoperative motor status.Spine J. 2024 Mar;24(3):506-518. doi: 10.1016/j.spinee.2023.10.009. Epub 2023 Oct 21. Spine J. 2024. PMID: 37871658
-
Effect of dexmedetomidine on evoked-potential monitoring in patients undergoing brain stem and supratentorial cranial surgery.Acta Anaesthesiol Scand. 2021 Sep;65(8):1043-1053. doi: 10.1111/aas.13835. Epub 2021 May 12. Acta Anaesthesiol Scand. 2021. PMID: 33884609 Clinical Trial.
-
Effects of Dexmedetomidine on motor- and somatosensory-evoked potentials in patients with thoracic spinal cord tumor: a randomized controlled trial.BMC Anesthesiol. 2016 Aug 2;16(1):51. doi: 10.1186/s12871-016-0217-y. BMC Anesthesiol. 2016. PMID: 27484701 Free PMC article. Clinical Trial.
-
Effects of dexmedetomidine on sevoflurane requirement for 50% excellent tracheal intubation in children: a randomized, double-blind comparison.Paediatr Anaesth. 2014 Sep;24(9):987-93. doi: 10.1111/pan.12430. Epub 2014 May 14. Paediatr Anaesth. 2014. PMID: 24823715 Review.
-
What is the predictive value of intraoperative somatosensory evoked potential monitoring for postoperative neurological deficit in cervical spine surgery?-a meta-analysis.Spine J. 2021 Apr;21(4):555-570. doi: 10.1016/j.spinee.2021.01.010. Epub 2021 Jan 16. Spine J. 2021. PMID: 33460808 Review.
Cited by
-
Effect of dexmedetomidine on somatosensory- and motor-evoked potentials in patients receiving craniotomy under propofol-sevoflurane combined anesthesia.Front Surg. 2024 Jul 9;11:1386049. doi: 10.3389/fsurg.2024.1386049. eCollection 2024. Front Surg. 2024. PMID: 39045089 Free PMC article.
-
The dose-dependent efficacy of esketamine in spinal surgery with intraoperative neuroelectrophysiological monitoring: a randomized controlled trial.Front Med (Lausanne). 2025 Jun 18;12:1579908. doi: 10.3389/fmed.2025.1579908. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40606459 Free PMC article.
-
Anesthesia and Pain Management for Scoliosis Surgery: A Narrative Review.Clin Spine Surg. 2025 Jul 1;38(6):259-265. doi: 10.1097/BSD.0000000000001758. Epub 2025 Jan 3. Clin Spine Surg. 2025. PMID: 39749911 Free PMC article. Review.
-
The Influence of Anesthesia on Neuromonitoring During Scoliosis Surgery: A Systematic Review.NeuroSci. 2024 Dec 17;5(4):693-712. doi: 10.3390/neurosci5040049. NeuroSci. 2024. PMID: 39728681 Free PMC article. Review.
-
Development and Internal Validation of Machine Learning to Predict Postoperative Worse Functional Status after Surgical Treatment for Thoracic Spinal Stenosis.Med Sci Monit. 2024 Sep 26;30:e945310. doi: 10.12659/MSM.945310. Med Sci Monit. 2024. PMID: 39323074 Free PMC article.
References
-
- Chin Ted Chong M., Anaes M. M, Fanzca, Manninen P., Frcpc M. D., Vanitha Sivanaser M., et al. (2014). Direct Comparison of the Effect of Desflurane and Sevoflurane on Intraoperative Motor-Evoked Potentials Monitoring. J. Neurosurg. Anesthesiol 26, 306–312. 10.1097/ANA.0000000000000041 - DOI - PubMed
-
- CoreyWalker H. J. K. T., Park P. (2020). Neuroanesthesia Guidelines for Optimizing Transcranial Motor Evoked Potentials Neuromonitoring during Deformity and Complex Spinal Surgery: A Delphi Consensus Study. SPINE. - PubMed
-
- Deiner S., Luo X., Lin H. M., Sessler D. I., Saager L., Sieber F. E., et al. (2017). Intraoperative Infusion of Dexmedetomidine for Prevention of Postoperative Delirium and Cognitive Dysfunction in Elderly Patients Undergoing Major Elective Noncardiac Surgery: A Randomized Clinical Trial. JAMA Surg. 152, e171505. 10.1001/jamasurg.2017.1505 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources