

Efficacy and safety of two incobotulinumtoxinA injection intervals in cervical dystonia patients with inadequate benefit from standard injection intervals of botulinum toxin: Phase 4, open-label, randomized, noninferiority study
- PMID: 35330880
- PMCID: PMC8938329
- DOI: 10.1016/j.prdoa.2022.100142
Efficacy and safety of two incobotulinumtoxinA injection intervals in cervical dystonia patients with inadequate benefit from standard injection intervals of botulinum toxin: Phase 4, open-label, randomized, noninferiority study
Abstract
IntroductionSome patients with cervical dystonia (CD) receiving long-term botulinum neurotoxin (BoNT) therapy report early waning of treatment benefit before the typical 12-week reinjection interval.
Methods: This phase 4, open-label, randomized, noninferiority study (CD Flex; NCT01486264) compared 2 incobotulinumtoxinA injection schedules (Short Flex: 8 ± 2 weeks; Long Flex: 14 ± 2 weeks) in CD patients. Previous BoNT-responsive subjects who reported acceptable clinical benefit lasting < 10 weeks were recruited. Efficacy and safety were evaluated after 8 injection cycles. The primary endpoint was change in Toronto Western Spasmodic Torticollis Rating Scale (TWSTRS) severity subscale 4 weeks after the eighth injection. Secondary endpoints included TWSTRS total and subscale scores. Immunogenicity was assessed in a subset of patients.
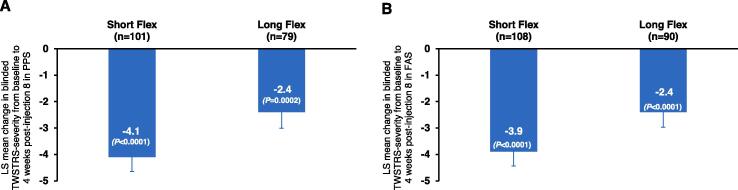
Results: Two hundred eighty-two CD patients were randomized and treated (Short Flex, N = 142; Long Flex, N = 140), and 207 completed the study. Significant improvements in TWSTRS severity from study baseline to 4 weeks after cycle 8 were observed in both the Short Flex (4.1 points; P < 0.0001) and Long Flex (2.4 points; P = 0.002) groups; Short Flex was noninferior to Long Flex (LS mean difference = 1.4 points; 95% CI = [-2.9, 0.1] < Δ = 2.0). Key secondary endpoints favored Short Flex intervals. Adverse events (AEs) were comparable between groups. There was no secondary loss of treatment effect.
Conclusion: Injection cycles < 10 weeks for incobotulinumtoxinA are effective (and noninferior to longer intervals) for treating CD patients with early waning of clinical benefit. Shorter injection intervals did not increase AEs or lead to loss of treatment effect.
Keywords: BoNT; Botulinum toxin; Cervical dystonia; IncobotulinumtoxinA; Movement disorders.
© 2022 Published by Elsevier Ltd.
Conflict of interest statement
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: Disclosures: Cynthia Comella serves on the editorial board of Clinical Neuropharmacology and Sleep Medicine. She has received compensation/honoraria for services as a consultant or an advisory committee member for Acadia Pharmaceuticals, Acorda Therapeutics, Adamas Pharmaceuticals, AEON Biopharma, Allergan, Ipsen Pharmaceuticals, Jazz Pharmaceuticals, Lundbeck, Merz Pharmaceuticals, Neurocrine Biosciences, Revance Therapeutics, and Sunovion Pharmaceuticals. She receives royalties from Wolters Kluwer. Robert Hauser has received consulting fees from AbbVie, Acadia, Acorda, Adamas, Alterity, Amneal, Aptinyx, Britannia, Cerevance, Curium Pharma, Enterin, Inhibikase, Jazz, KeiferRx, Kyowa Kirin, Lundbeck A/S, Merck, Merz, Neurocrine Biosciences, Novus, Pharma Two B, Pharmather, Revance Therapeutics, Roche, Sage Therapeutics, Scion NeuroStim, Sio Gene Therapies, Sunovion, Supernus, Tolmar, US WorldMeds, and Vivifi Biotech and has received speaker fees from AbbVie, Acorda, Adamas, Amneal, Kyowa Kirin, Neurocrine Biosciences, and Sunovion. He holds stock in Axial Biotherapeutics and Inhibikase. His institution, University of South Florida, received research fees from AbbVie, Axovant Sciences, Biogen, Bukwang Pharmaceuticals, Cavion, Centogene, Cerevance, Cerevel Therapeutics, Cynapsus Therapeutics, Enterin, F. Hoffmann-La Roche, Genentech, Global Kinetics Corporation, Impax Specialty Pharma, Intec Pharma, Integrative Research Laboratories Sweden AB, Jazz Pharmaceuticals, MJFF, Neuraly, NeuroDerm, Neurocrine Biosciences, Northwestern University, Pfizer, Pharma Two B, Revance Therapeutics, Sanofi US Services, Sun Pharma Advanced Research Company, Sunovion Pharmaceuticals, and UCB Biopharma SPRL. Stuart Isaacson has received honoraria for CME for, was a consultant for, received research grants from, and/or was a promotional speaker on behalf of Abbvie, Allergan, Ipsen, Merz, Revance, Supernus, and US World Meds. Daniel Truong has received research funding from Abbvie, Acorda, Aeon, Auspex, Biogen, Bukwang, Cerevel, Cynapsus, Daiichi Sankyo Pharma, Eli Lilly, Enterin, Ipsen, Kyowa, Lundbeck, Merz, National Institute of Neurological Disorders and Stroke, Neurocrine, Neuroderm, Parkinson’s Foundation, Prilenia, Revance, and Sunovion. He has received honoraria for consulting and speaker activities from Acorda, Neurocrine, TEVA, an US Worldmed. Odinachi Oguh is a paid speaker and consultant for Sunovion Pharmaceuticals. Jennifer Hui is an advisory board member for Acorda, serves as a consultant for Sunovion, and receives grant support from Roche. Eric Molho is on the speakers bureau for Neurocrine Biosciences; received research funding from Amneal Pharmaceuticals, Biohaven Pharmaceuticals, Cerevel Therapeutics, CHDI/HSG, and Enterin; and received educational grants from AbbVie and Merz Pharmaceuticals. Matthew Brodsky has no conflicts of interest to disclose. Erin Furr-Stimming receives research funding from Cures within Reach, HDSA, Neurocrine, Prilenia, Roche/Genetech, and Uniqure; has consulted for Teva; and is on the speakers bureau for Sunovion; none of these are related to Xeomin or conflict with work being presented. Georg Comes and Michael Hast and are employees of Merz Pharmaceuticals. David Charles received income from Alliance for Patient Access, Merz, Newronika, Revance, and Supernus for consulting services. His institution, Vanderbilt University Medical Center, receives income from grants or contracts with Abbott, AbbVie, Aeon, Boston Scientific, Impax, Intec, Ipsen, Lundbeck, Medtronic, Merz, Novartis, Pharma Two B, and Supernus for research or educational programs that he has led.
Figures
Similar articles
-
A randomized, double-blind study of repeated incobotulinumtoxinA (Xeomin(®)) in cervical dystonia.J Neural Transm (Vienna). 2013 Dec;120(12):1699-707. doi: 10.1007/s00702-013-1048-3. Epub 2013 Jun 19. J Neural Transm (Vienna). 2013. PMID: 23779062 Free PMC article. Clinical Trial.
-
Efficacy and safety of abobotulinumtoxinA liquid formulation in cervical dystonia: A randomized-controlled trial.Mov Disord. 2016 Nov;31(11):1649-1657. doi: 10.1002/mds.26760. Epub 2016 Sep 21. Mov Disord. 2016. PMID: 27653448 Clinical Trial.
-
Long-term efficacy and safety of incobotulinumtoxinA injections in patients with cervical dystonia.J Neurol Neurosurg Psychiatry. 2013 Sep;84(9):1014-9. doi: 10.1136/jnnp-2012-303608. Epub 2013 May 18. J Neurol Neurosurg Psychiatry. 2013. PMID: 23687362 Free PMC article. Clinical Trial.
-
Clinical and pharmacological properties of incobotulinumtoxinA and its use in neurological disorders.Drug Des Devel Ther. 2015 Apr 1;9:1913-26. doi: 10.2147/DDDT.S79193. eCollection 2015. Drug Des Devel Ther. 2015. PMID: 25897202 Free PMC article. Review.
-
Is it time for flexibility in botulinum inter-injection intervals?Toxicon. 2015 Dec 1;107(Pt A):72-6. doi: 10.1016/j.toxicon.2015.09.037. Epub 2015 Oct 9. Toxicon. 2015. PMID: 26440738 Review.
Cited by
-
Efficacy and safety of botulinum toxin for treating motor dysfunction in patients with Parkinson's disease: a systematic review and meta-analysis.BMJ Open. 2023 Jun 16;13(6):e060274. doi: 10.1136/bmjopen-2021-060274. BMJ Open. 2023. PMID: 37328181 Free PMC article.
-
Pain Reduction in Cervical Dystonia Following Treatment with IncobotulinumtoxinA: A Pooled Analysis.Toxins (Basel). 2023 May 12;15(5):333. doi: 10.3390/toxins15050333. Toxins (Basel). 2023. PMID: 37235367 Free PMC article.
-
Pooled Safety Analysis of IncobotulinumtoxinA in the Treatment of Neurological Disorders in Adults.Toxins (Basel). 2023 May 23;15(6):353. doi: 10.3390/toxins15060353. Toxins (Basel). 2023. PMID: 37368654 Free PMC article.
-
Patient Characteristics and Real-World Use of Botulinum Toxins for the Treatment of Cervical Dystonia, Blepharospasm, and Hemifacial Spasm.Toxins (Basel). 2024 Aug 16;16(8):362. doi: 10.3390/toxins16080362. Toxins (Basel). 2024. PMID: 39195772 Free PMC article.
-
Improving the Efficacy of Botulinum Toxin for Cervical Dystonia: A Scoping Review.Toxins (Basel). 2023 Jun 9;15(6):391. doi: 10.3390/toxins15060391. Toxins (Basel). 2023. PMID: 37368692 Free PMC article.
References
-
- Chan J., Brin M.F., Fahn S. Idiopathic cervical dystonia: clinical characteristics. Mov. Disord. 1991;6(2):119–126. - PubMed
-
- Molho E.S., Agarwal N., Regan K., Higgins D.S., Factor S.A. Effect of cervical dystonia on employment: a retrospective analysis of the ability of treatment to restore premorbid employment status. Mov. Disord. 2009;24:1384–1387. - PubMed
-
- Simpson D.M., Hallett M., Ashman E.J., Comella C.L., Green M.W., Gronseth G.S., et al. Practice guideline update summary: botulinum neurotoxin for the treatment of blepharospasm, cervical dystonia, adult spasticity, and headache: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2016;86:1818–1826. - PMC - PubMed
-
- Greene P., Fahn S., Diamond B. Development of resistance to botulinum toxin type A in patients with torticollis. Mov. Disord. 1994;9(2):213–217. - PubMed
