

Strategy to Reduce Hypercapnia in Robot-Assisted Radical Prostatectomy Using Transcutaneous Carbon Dioxide Monitoring: A Prospective Observational Study
- PMID: 35330918
- PMCID: PMC8938168
- DOI: 10.2147/TCRM.S347690
Strategy to Reduce Hypercapnia in Robot-Assisted Radical Prostatectomy Using Transcutaneous Carbon Dioxide Monitoring: A Prospective Observational Study
Abstract
Purpose: Monitoring end-tidal carbon dioxide partial pressure (PETCO2) is a noninvasive, continuous method, but its accuracy is reduced by prolonged capnoperitoneum and the steep Trendelenburg position in robot-assisted radical prostatectomy (RARP). Transcutaneous carbon dioxide partial pressure (PTCCO2) monitoring, which is not affected by ventilator-perfusion mismatch, has been suggested as a suitable alternative. We compared the agreement of noninvasive measurements with the arterial carbon dioxide partial pressure (PaCO2) over a long period of capnoperitoneum, and investigated its sensitivity and predictive power for detecting hypercapnia.
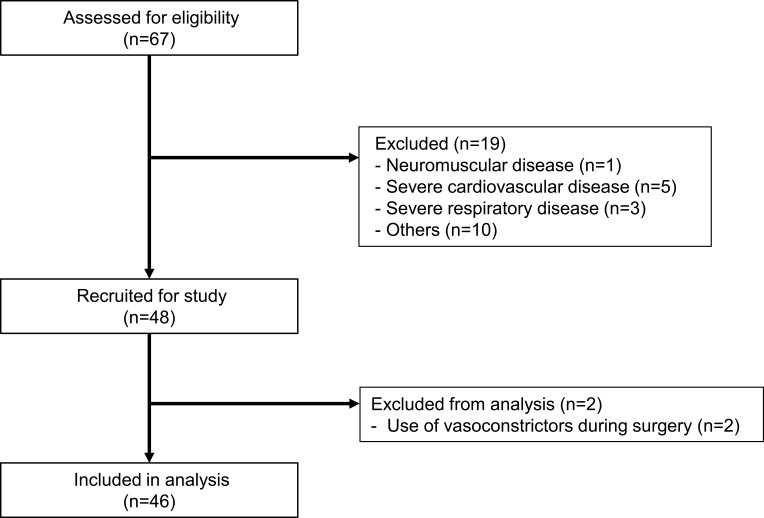
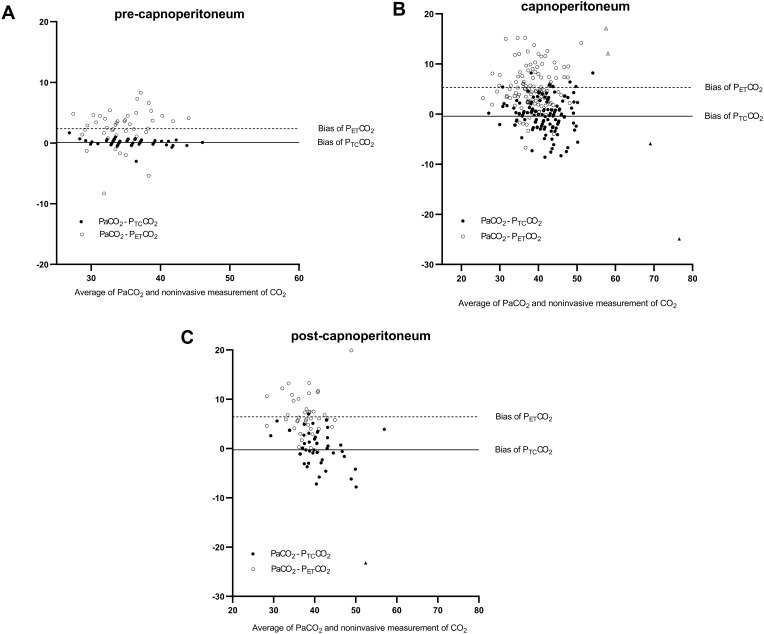
Patients and methods: The patients who underwent RARP were enrolled in this study prospectively. Intraoperative measurements of PETCO2, PTCCO2, and PaCO2 were analyzed. The primary outcome was the agreement of noninvasive monitoring with PaCO2 during prolonged capnoperitoneum. Bias and precision between noninvasive measurements and PaCO2 were assessed using Bland-Altman analysis. The bias and mean absolute difference were compared using a two-tailed Wilcoxon signed-rank test for pairs. The secondary outcome was the sensitivity and predictive power for detecting hypercapnia. To assess this, the Yates corrected chi-square test and the area under the receiver operating characteristic curve were used.
Results: The study analyzed 219 datasets from 46 patients. Compared with PETCO2, PTCCO2 had lower bias, greater precision, and better agreement with PaCO2 throughout the RARP. The mean absolute difference in PETCO2 and PaCO2 was larger than that of PTCCO2 and PaCO2, and continued to exceed the clinically acceptable range of 5 mmHg after 1 hour of capnoperitoneum. The sensitivity during capnoperitoneum and overall predictive power of PTCCO2 for detecting hypercapnia were significantly higher than those of PETCO2, suggesting a greater contribution to ventilator adjustment, to treat hypercapnia.
Conclusion: PTCCO2 monitoring measured PaCO2 more accurately than PETCO2 monitoring during RARP requiring prolonged capnoperitoneum and a steep Trendelenburg position. PTCCO2 monitoring also provides more sensitive measurements for ventilator adjustment and detects hypercapnia more effectively than PETCO2 monitoring.
Keywords: capnoperitoneum; end-tidal carbon dioxide monitoring; general anesthesia; intraoperative carbon dioxide monitoring; robotic surgery.
© 2022 Lee et al.
Conflict of interest statement
All authors report no conflicts of interest arising from this work.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
