

An integrated modelling methodology for estimating global incidence and prevalence of hereditary spastic paraplegia subtypes SPG4, SPG7, SPG11, and SPG15
- PMID: 35331153
- PMCID: PMC8944001
- DOI: 10.1186/s12883-022-02595-4
An integrated modelling methodology for estimating global incidence and prevalence of hereditary spastic paraplegia subtypes SPG4, SPG7, SPG11, and SPG15
Abstract
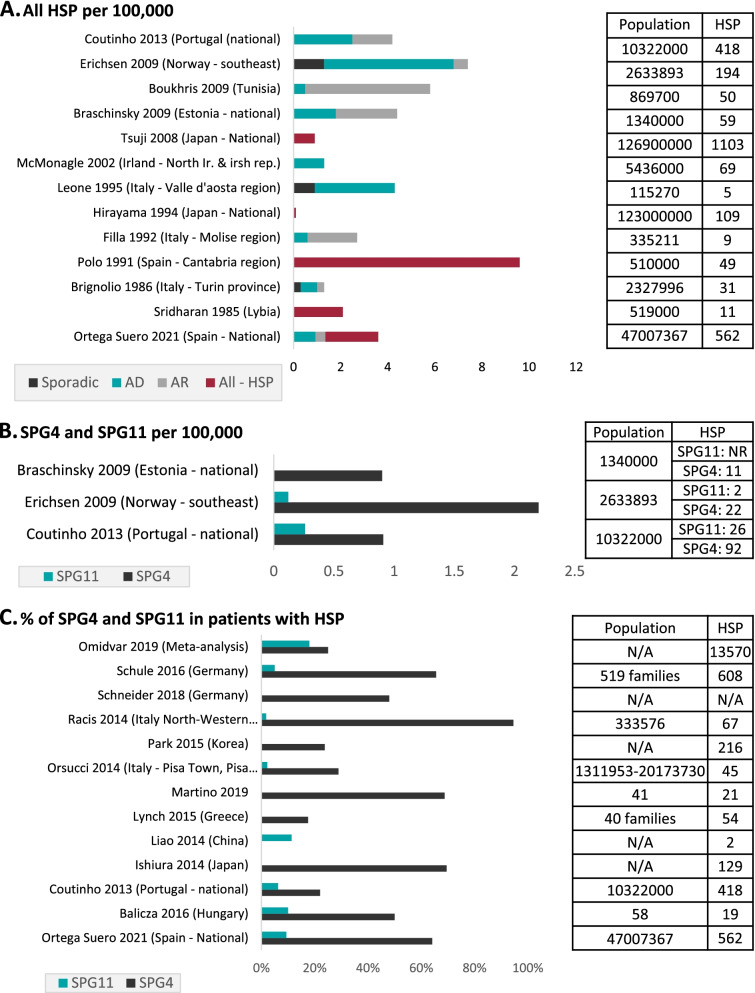
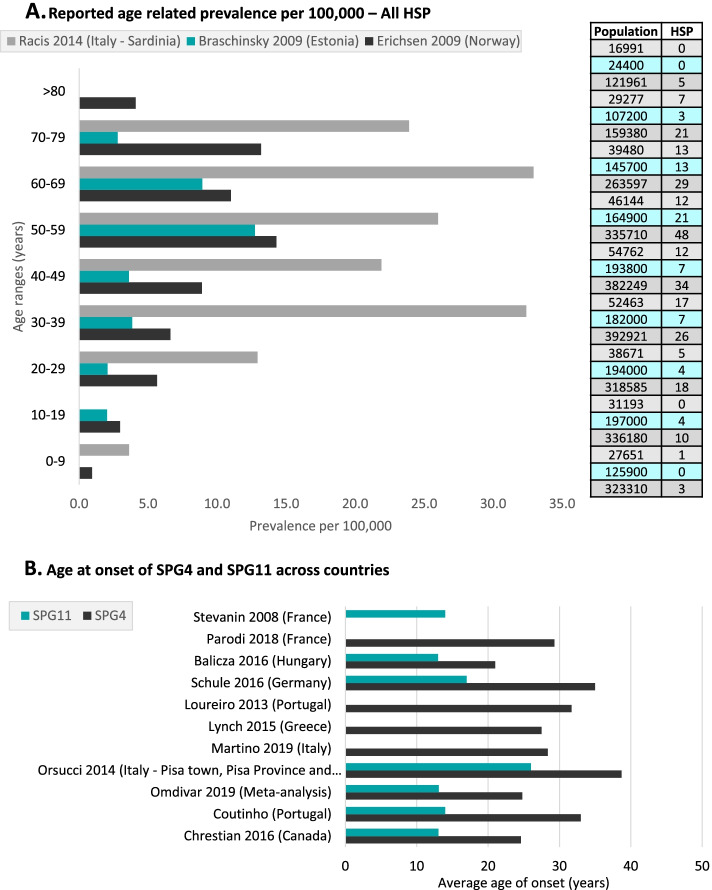
Background: Hereditary spastic paraplegias (HSPs) are progressively debilitating neurodegenerative disorders that follow heterogenous patterns of Mendelian inheritance. Available epidemiological evidence provides limited incidence and prevalence data, especially at the genetic subtype level, preventing a realistic estimation of the true social burden of the disease. The objectives of this study were to (1) review the literature on epidemiology of HSPs; and (2) develop an epidemiological model of the prevalence of HSP, focusing on four common HSP genetic subtypes at the country and region-level.
Methods: A model was constructed estimating the incidence at birth, survival, and prevalence of four genetic subtypes of HSP based on the most appropriate published literature. The key model parameters were assessed by HSP clinical experts, who provided feedback on the validity of assumptions. A model was then finalized and validated through comparison of outputs against available evidence. The global, regional, and national prevalence and patient pool were calculated per geographic region and per genetic subtype.
Results: The HSP global prevalence was estimated to be 3.6 per 100,000 for all HSP forms, whilst the estimated global prevalence per genetic subtype was 0.90 (SPG4), 0.22 (SPG7), 0.34 (SPG11), and 0.13 (SPG15), respectively. This equates to an estimated 3365 (SPG4) and 872 (SPG11) symptomatic patients, respectively, in the USA.
Conclusions: This is the first epidemiological model of HSP prevalence at the genetic subtype-level reported at multiple geographic levels. This study offers additional data to better capture the burden of illness due to mutations in common genes causing HSP, that can inform public health policy and healthcare service planning, especially in regions with higher estimated prevalence of HSP.
Keywords: Epidemiological model; Epidemiology; Hereditary spastic paraplegia; Incidence; Prevalence.
© 2022. The Author(s).
Conflict of interest statement
B.S.C. is a cofounder of Dynacure. C.F., L.T., S.v.R., S.H., are consultants or currently employed by Dynacure, and A.D., R.S., and C.Bl. are currently on the medical advisory board. G.V.S, G.E., C.Bu., I.O. are consultants or employees of ISMS, hired by Dynacure to perform this work.
Figures




References
-
- Erfanian Omidvar M, Torkamandi S, Rezaei S, Alipoor B, Omrani MD, Darvish H, et al. Genotype–phenotype associations in hereditary spastic paraplegia: a systematic review and meta-analysis on 13,570 patients. J Neurol. 2021;268:2065–2082. - PubMed
-
- Ruano L, Melo C, Silva MC, Coutinho P. The global epidemiology of hereditary ataxia and spastic paraplegia: a systematic review of prevalence studies. Neuroepidemiology. 2014;42:174–183. - PubMed
-
- Stevanin G, Azzedine H, Denora P, Boukhris A, Tazir M, Lossos A, et al. Mutations in SPG11 are frequent in autosomal recessive spastic paraplegia with thin corpus callosum, cognitive decline and lower motor neuron degeneration. Brain. 2008;131:772–784. - PubMed
-
- Parodi L, Fenu S, Barbier M, Banneau G, Duyckaerts C, du Montcel ST, et al. Spastic paraplegia due to SPAST mutations is modified by the underlying mutation and sex. Brain. 2018;141:3331–3342. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
