

Proteomic signature of tubulointerstitial tissue predicts prognosis in IgAN
- PMID: 35331167
- PMCID: PMC8943973
- DOI: 10.1186/s12882-022-02736-4
Proteomic signature of tubulointerstitial tissue predicts prognosis in IgAN
Abstract
Background: IgA nephropathy (IgAN) is associated with a significant risk of progression to kidney failure. Tubular atrophy is an established important risk factor for progressive disease, but few studies have investigated tubulointerstitial molecular markers and mechanisms of progression in IgAN.
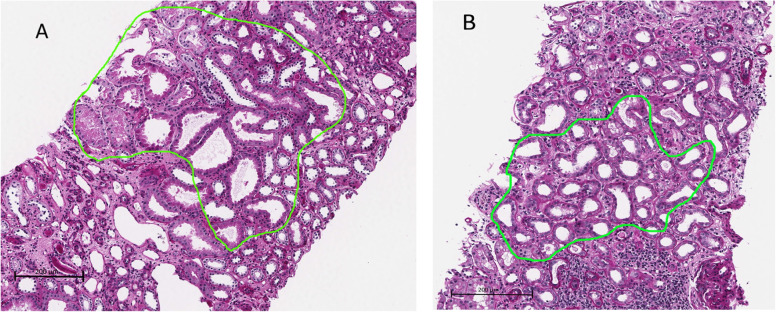
Methods: Based on data from the Norwegian Renal Registry, two groups were included: IgAN patients with (n = 9) or without (n = 18) progression to kidney failure during 10 years of follow-up. Tubulointerstitial tissue without discernible interstitial expansion or pronounced tubular alterations was microdissected, proteome was analysed using tandem mass spectrometry and relative protein abundances were compared between groups.
Results: Proteome analyses quantified 2562 proteins with at least 2 unique peptides. Of these, 150 proteins had significantly different abundance between progressive and non-progressive IgAN patients, 67 were more abundant and 83 less abundant. Periostin was the protein with the highest fold change between progressive and non-progressive IgAN (fold change 8.75, p < 0.05) and periostin staining was also stronger in patients with progressive vs non-progressive IgAN. Reactome pathway analyses showed that proteins related to inflammation were more abundant and proteins involved in mitochondrial translation were significantly less abundant in progressive vs non-progressive patients.
Conclusions: Microdissection of tubulointerstitial tissue with only mild damage allowed for identification of proteome markers of early progressive IgAN. Periostin abundance showed promise as a novel and important risk marker of progression.
Keywords: ESRD; Formalin-fixed paraffin embedded kidney biopsy tissue; IgA nephropathy; Liquid chromatography–tandem mass spectrometry; Proteomic analyses; Tubulointerstitium.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



References
-
- Roberts IS, Cook HT, Troyanov S, Alpers CE, Amore A, Barratt J, Berthoux F, Bonsib S, Bruijn JA, Cattran DC, Coppo R, D’Agati V, D’Amico G, Emancipator S, Emma F, Feehally J, Ferrario F, Fervenza FC, Florquin S, Fogo A, Geddes CC, Groene HJ, Haas M, Herzenberg AM, Hill PA, Hogg RJ, Hsu SI, Jennette JC, Joh K, Julian BA, Kawamura T, Lai FM, Li LS, Li PK, Liu ZH, Mackinnon B, Mezzano S, Schena FP, Tomino Y, Walker PD, Wang H, Weening JJ, Yoshikawa N, Zhang H. The Oxford classification of IgA nephropathy: pathology definitions, correlations, and reproducibility. Kidney Int. 2009;76:546–56. - PubMed
-
- Lai KN, Chan LY, Leung JC. Mechanisms of tubulointerstitial injury in IgA nephropathy. Kidney Int Suppl. 2005;94:S110–115. - PubMed
-
- Liu BC, Tang TT, Lv LL. How Tubular Epithelial Cell Injury Contributes to Renal Fibrosis. Adv Exp Med Biol. 2019;1165:233–252. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
