

Early prone positioning in acute respiratory distress syndrome related to COVID-19: a propensity score analysis from the multicentric cohort COVID-ICU network-the ProneCOVID study
- PMID: 35331332
- PMCID: PMC8944409
- DOI: 10.1186/s13054-022-03949-7
Early prone positioning in acute respiratory distress syndrome related to COVID-19: a propensity score analysis from the multicentric cohort COVID-ICU network-the ProneCOVID study
Abstract
Background: Delaying time to prone positioning (PP) may be associated with higher mortality in acute respiratory distress syndrome (ARDS) due to coronavirus disease 2019 (COVID-19). We evaluated the use and the impact of early PP on clinical outcomes in intubated patients hospitalized in intensive care units (ICUs) for COVID-19.
Methods: All intubated patients with ARDS due to COVID-19 were involved in a secondary analysis from a prospective multicenter cohort study of COVID-ICU network including 149 ICUs across France, Belgium and Switzerland. Patients were followed-up until Day-90. The primary outcome was survival at Day-60. Analysis used a Cox proportional hazard model including a propensity score.
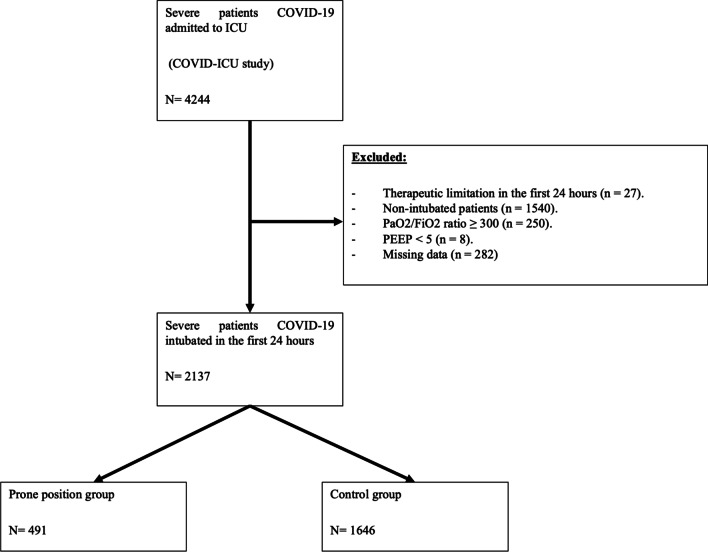
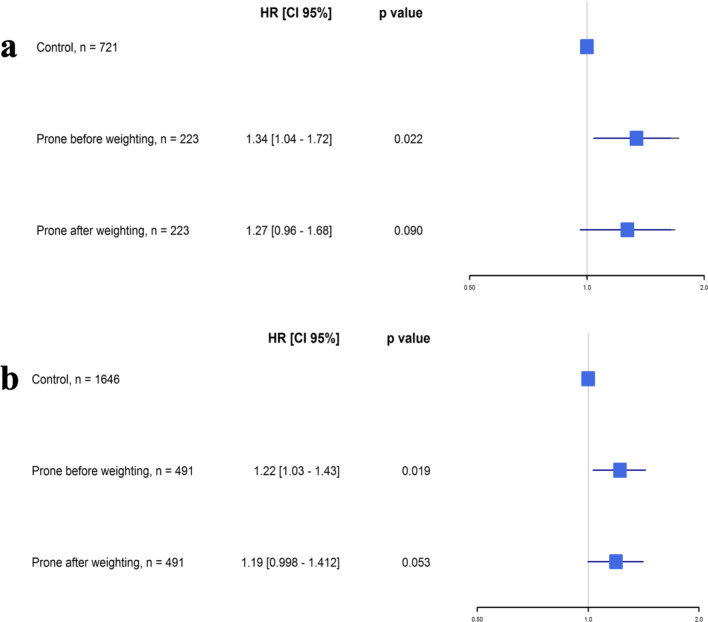
Results: Among 2137 intubated patients, 1504 (70.4%) were placed in PP during their ICU stay and 491 (23%) during the first 24 h following ICU admission. One hundred and eighty-one patients (36.9%) of the early PP group had a PaO2/FiO2 ratio > 150 mmHg when prone positioning was initiated. Among non-early PP group patients, 1013 (47.4%) patients had finally been placed in PP within a median delay of 3 days after ICU admission. Day-60 mortality in non-early PP group was 34.2% versus 39.3% in the early PP group (p = 0.038). Day-28 and Day-90 mortality as well as the need for adjunctive therapies was more important in patients with early PP. After propensity score adjustment, no significant difference in survival at Day-60 was found between the two study groups (HR 1.34 [0.96-1.68], p = 0.09 and HR 1.19 [0.998-1.412], p = 0.053 in complete case analysis or in multiple imputation analysis, respectively).
Conclusions: In a large multicentric international cohort of intubated ICU patients with ARDS due to COVID-19, PP has been used frequently as a main treatment. In this study, our data failed to show a survival benefit associated with early PP started within 24 h after ICU admission compared to PP after day-1 for all COVID-19 patients requiring invasive mechanical ventilation regardless of their severity.
Keywords: Acute respiratory distress syndrome; COVID-19; Intensive care unit; Intubation; Mortality; Prone position.
© 2022. The Author(s).
Conflict of interest statement
All authors declare no competing interests.
Figures

References
-
- World Health Organization. Coronarovirus (COVID-19) dashboard. Available at https://covid19.who.int. Accessed 12 May 2022.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
