

Coronary Risk Estimation Based on Clinical Data in Electronic Health Records
- PMID: 35331410
- PMCID: PMC8956801
- DOI: 10.1016/j.jacc.2022.01.021
Coronary Risk Estimation Based on Clinical Data in Electronic Health Records
Abstract
Background: Clinical features from electronic health records (EHRs) can be used to build a complementary tool to predict coronary artery disease (CAD) susceptibility.
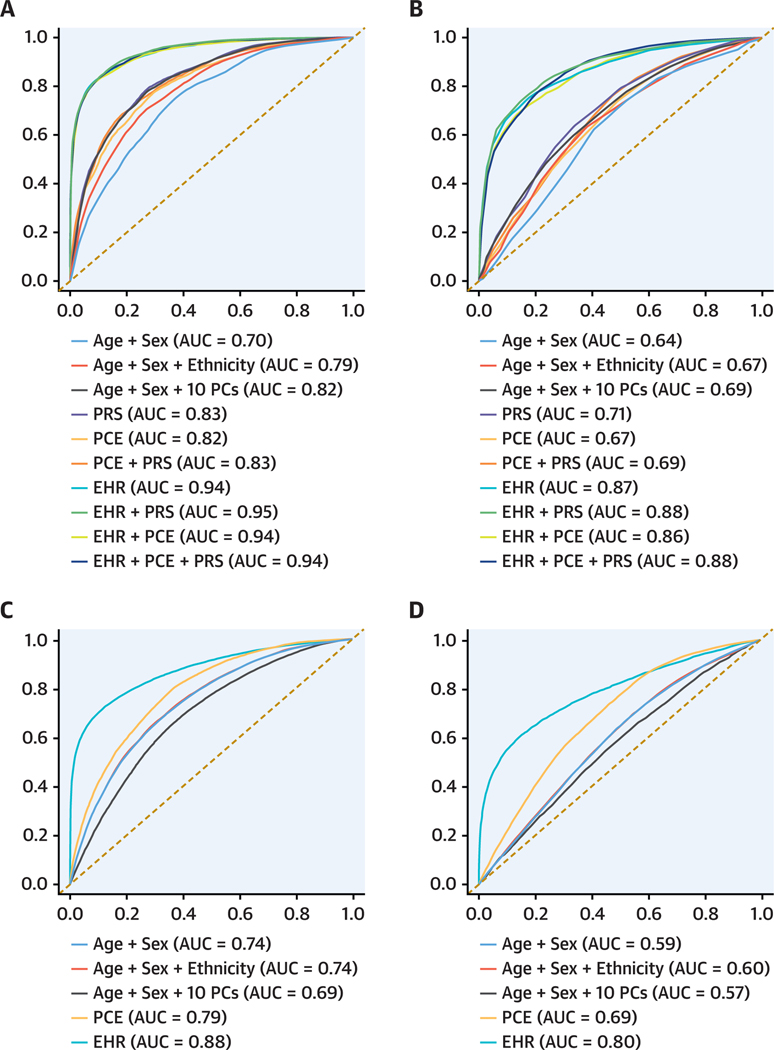
Objectives: The purpose of this study was to determine whether an EHR score can improve CAD prediction and reclassification 1 year before diagnosis, beyond conventional clinical guidelines as determined by the pooled cohort equations (PCE) and a polygenic risk score for CAD.
Methods: We applied a machine learning framework using clinical features from the EHR in a multiethnic, clinical care cohort (BioMe) comprising 555 CAD cases and 6,349 control subjects and in a population-based cohort (UK Biobank) comprising 3,130 CAD cases and 378,344 control subjects for external validation.
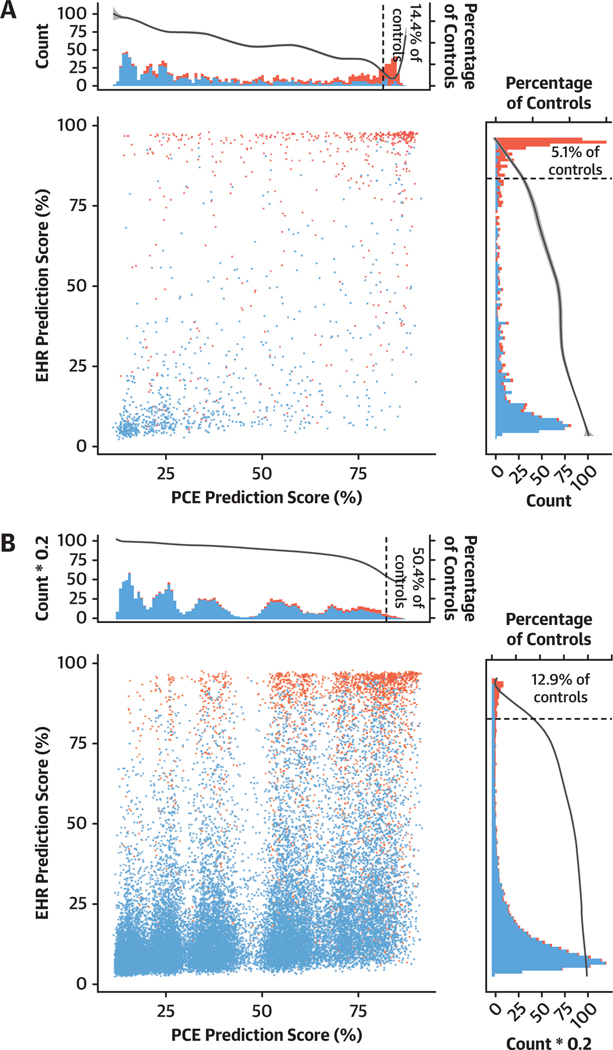
Results: Compared with the PCE, the EHR score improved CAD prediction by 12% in the BioMe Biobank and by 9% in the UK Biobank. The EHR score reclassified 25.8% and 15.2% individuals in each cohort respectively, compared with the PCE score. We observed larger improvements in the EHR score over the PCE in a subgroup of individuals with low CAD risk, with 20% increased discrimination and 34.4% increased reclassification. In all models, the polygenic risk score for CAD did not improve CAD prediction, compared with the PCE or EHR score.
Conclusions: The EHR score resulted in increased prediction and reclassification for CAD, demonstrating its potential use for population health monitoring of short-term CAD risk in large health systems.
Keywords: biobank; coronary artery disease; electronic health record; machine learning; polygenic risk score; pooled cohort equations; prevention.
Copyright © 2022 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures Mr Forrest is supported by the National Institute of General Medical Sciences of the National Institutes of Health (NIH) (T32-GM007280). Dr Nadkarni is supported by a career development award from the NIH (K23-DK107908) and by NIH grants (R01-DK108803, U01-HG007278, U01-HG009610, and U01-DK116100); is scientific cofounder, consultant, advisory board member, and equity owner of Renalytix AI; is a scientific cofounder and equity holder for Pensieve Health; has served as a consultant for Variant Bio; has received grants from Goldfinch Bio; and has received personal fees from Renalytix AI, BioVie, Reata, AstraZeneca, and GLG Consulting. Dr Do is supported by the National Institute of General Medical Sciences of the NIH (R35-GM124836) and the National Heart, Lung, and Blood Institute of the NIH (R01-HL139865 and R01-HL155915); has received grants from AstraZeneca; has received grants and nonfinancial support from Goldfinch Bio; is a scientific cofounder, consultant, and equity holder for Pensieve Health; and has served as a consultant for Variant Bio. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Figures


Comment in
-
Big Data and ASCVD Risk Prediction: Building a Better Mouse Trap?J Am Coll Cardiol. 2022 Mar 29;79(12):1167-1169. doi: 10.1016/j.jacc.2022.01.020. J Am Coll Cardiol. 2022. PMID: 35331411 No abstract available.
Similar articles
-
Polygenic risk score improves the accuracy of a clinical risk score for coronary artery disease.BMC Med. 2022 Nov 7;20(1):385. doi: 10.1186/s12916-022-02583-y. BMC Med. 2022. PMID: 36336692 Free PMC article.
-
Predictive Accuracy of a Polygenic Risk Score-Enhanced Prediction Model vs a Clinical Risk Score for Coronary Artery Disease.JAMA. 2020 Feb 18;323(7):636-645. doi: 10.1001/jama.2019.22241. JAMA. 2020. PMID: 32068818 Free PMC article.
-
Integrated Polygenic Tool Substantially Enhances Coronary Artery Disease Prediction.Circ Genom Precis Med. 2021 Apr;14(2):e003304. doi: 10.1161/CIRCGEN.120.003304. Epub 2021 Mar 2. Circ Genom Precis Med. 2021. PMID: 33651632 Free PMC article.
-
Nonobstructive Coronary Artery Disease by Coronary CT Angiography Improves Risk Stratification and Allocation of Statin Therapy.JACC Cardiovasc Imaging. 2017 Sep;10(9):1031-1038. doi: 10.1016/j.jcmg.2016.10.022. Epub 2017 Mar 15. JACC Cardiovasc Imaging. 2017. PMID: 28330658 Free PMC article. Review.
-
Genome-Wide Association Studies and Risk Scores for Coronary Artery Disease: Sex Biases.Adv Exp Med Biol. 2018;1065:627-642. doi: 10.1007/978-3-319-77932-4_38. Adv Exp Med Biol. 2018. PMID: 30051411 Review.
Cited by
-
Immune-related risk score: An immune-cell-pair-based prognostic model for cutaneous melanoma.Front Immunol. 2023 Feb 15;14:1112181. doi: 10.3389/fimmu.2023.1112181. eCollection 2023. Front Immunol. 2023. PMID: 36875110 Free PMC article.
-
Machine learning based prediction models for cardiovascular disease risk using electronic health records data: systematic review and meta-analysis.Eur Heart J Digit Health. 2024 Oct 27;6(1):7-22. doi: 10.1093/ehjdh/ztae080. eCollection 2025 Jan. Eur Heart J Digit Health. 2024. PMID: 39846062 Free PMC article. Review.
-
Short-term prediction of coronary artery disease using serum metabolomic patterns.Am Heart J Plus. 2022 Dec;24:100232. doi: 10.1016/j.ahjo.2022.100232. Epub 2022 Nov 23. Am Heart J Plus. 2022. PMID: 36788979 Free PMC article. No abstract available.
-
UKB-MDRMF: a multi-disease risk and multimorbidity framework based on UK biobank data.Nat Commun. 2025 Apr 22;16(1):3767. doi: 10.1038/s41467-025-58724-3. Nat Commun. 2025. PMID: 40263246 Free PMC article.
-
Machine learning-based marker for coronary artery disease: derivation and validation in two longitudinal cohorts.Lancet. 2023 Jan 21;401(10372):215-225. doi: 10.1016/S0140-6736(22)02079-7. Epub 2022 Dec 20. Lancet. 2023. PMID: 36563696 Free PMC article.
References
-
- Zamorano JL, del Val D. Predictive models of atherosclerotic cardiovascular disease: in search of the philosopher’s stone of cardiology. J Am Coll Cardiol. 2016;67:148–150. - PubMed
-
- Stone NJ, Robinson JG, Lichtenstein AH, et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63(25 Pt B):2889–2934. - PubMed
-
- Ridker PM, Cook NR. Statins: new American guidelines for prevention of cardiovascular disease. Lancet. 2013;382:1762–1765. - PubMed
-
- Kavousi M, Leening MJG, Nanchen D, et al..Comparison of application of the ACC/AHA Guidelines, Adult Treatment Panel III Guidelines, and European Society of Cardiology Guidelines for Cardiovascular Disease Prevention in a European cohort. JAMA. 2014;311:1416–1423. - PubMed
Publication types
MeSH terms
Grants and funding
- R35 GM124836/GM/NIGMS NIH HHS/United States
- U01 HG009610/HG/NHGRI NIH HHS/United States
- R01 HL139865/HL/NHLBI NIH HHS/United States
- S10 OD026880/OD/NIH HHS/United States
- U01 HG007278/HG/NHGRI NIH HHS/United States
- T32 HL007824/HL/NHLBI NIH HHS/United States
- R01 DK108803/DK/NIDDK NIH HHS/United States
- S10 OD030463/OD/NIH HHS/United States
- T32 GM007280/GM/NIGMS NIH HHS/United States
- R01 HL155915/HL/NHLBI NIH HHS/United States
- K23 DK107908/DK/NIDDK NIH HHS/United States
- U01 DK116100/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
