

The modified NUTRIC score (mNUTRIC) is associated with increased 28-day mortality in critically ill COVID-19 patients: Internal validation of a prediction model
- PMID: 35331492
- PMCID: PMC8849901
- DOI: 10.1016/j.clnesp.2022.02.014
The modified NUTRIC score (mNUTRIC) is associated with increased 28-day mortality in critically ill COVID-19 patients: Internal validation of a prediction model
Abstract
Background: High prevalence of malnutrition was found in critically ill COVID-19 patients. The modified Nutrition Risk in the Critically ill (mNUTRIC) score is frequently used for nutritional risk assessment in intensive care unit (ICU) COVID-19 patients. The aim of this study was to investigate the role of mNUTRIC score to predict 28-day mortality in critically ill COVID-19 patients admitted to ICU.
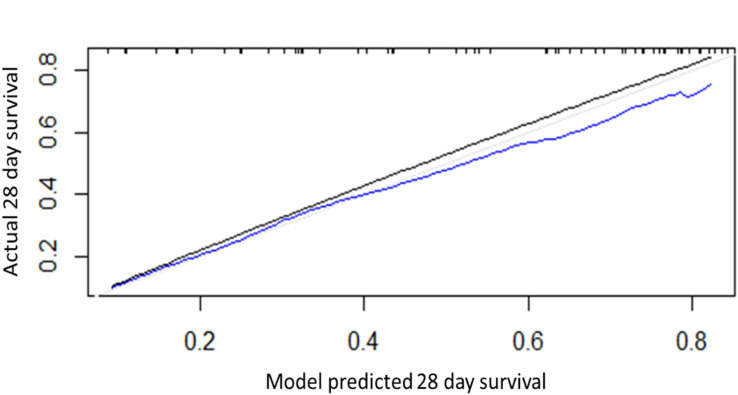
Methods: A cohort of consecutive COVID-19 critically ill patients admitted to ICU was retrospectively evaluated and the nutritional risk was assessed with the use of mNUTRIC score. A multivariable Cox regression model to predict 28-day mortality was therefore developed including the mNUTRIC as a covariate. Internal validation was performed using the bootstrap resampling technique to reduce possible bias in the estimated risks. The performance of the prediction model was assessed via calibration and discrimination.
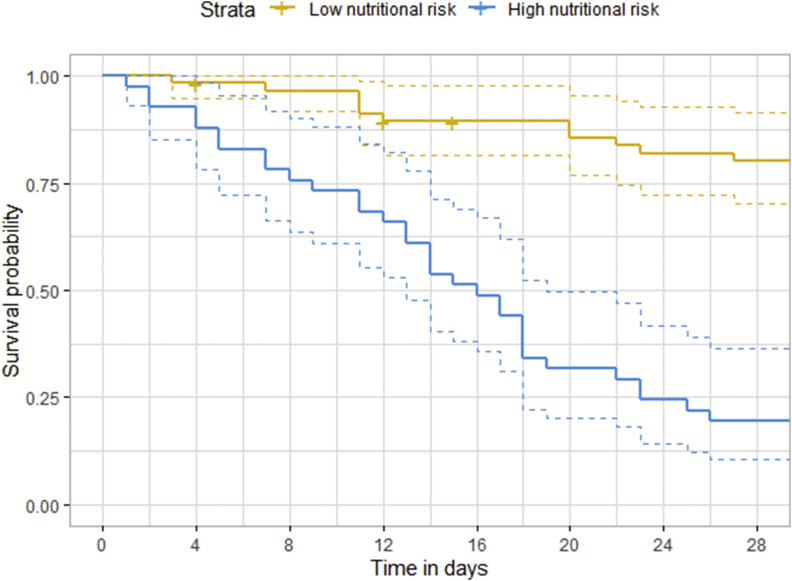
Results: A total of 98 critically ill COVID-19 patients with a median age of 66 years (56-73 IQR), 81 (82.7%) males were included in this study. A high nutritional risk (mNUTRIC ≥5 points) was observed in 41.8% of our critically ill COVID-19 patients while a low nutritional risk (mNUTRIC <5 points) was observed in 58.2%. Forty-five patients (45.9%) died within 28 days after ICU admission. In multivariable model after internal validation, mNUTRIC ≥5 (optimism adjusted HR 2.38, 95% CI 1.08-5.25, p = 0.02) and high-sensitivity C-reactive protein values (CRP) (optimism adjusted HR 1.02, 95% CI 1.01-1.07, p = 0.005) were independent predictors of 28-day mortality.
Conclusions: A high prevalence of malnutrition as revealed by mNUTRIC was found in our critically ill COVID-19 patients once admitted in ICU. After adjustment for covariables, mNUTRIC ≥5 and CRP levels were independently associated with 28-day mortality in critically ill COVID-19 patients. The final model revealed good discrimination and calibration. Nutritional risk assessment is essential for the management of critically ill COVID-19 patients as well as for outcome prediction.
Keywords: Coronavirus disease 2019 (COVID-19); Intensive care unit; Modified NUTRIC score (mNUTRIC); Mortality; Nutritional risk assessment.
Copyright © 2022. Published by Elsevier Ltd.
Conflict of interest statement
Declaration of competing interest The authors certify that they have no affiliation with, or involvement in any organization or entity with any financial or non-financial interest in the subject matter discussed in this manuscript.
Figures
Similar articles
-
The modified NUTRIC score can be used for nutritional risk assessment as well as prognosis prediction in critically ill COVID-19 patients.Clin Nutr. 2021 Feb;40(2):534-541. doi: 10.1016/j.clnu.2020.05.051. Epub 2020 Jun 5. Clin Nutr. 2021. PMID: 32527576 Free PMC article.
-
Comparison of nutritional risk status assessment tools in predicting 30-day survival in critically ill COVID-19 pneumonia patients.Ann Saudi Med. 2022 Jul-Aug;42(4):236-245. doi: 10.5144/0256-4947.2022.236. Epub 2022 Aug 4. Ann Saudi Med. 2022. PMID: 35933605 Free PMC article.
-
Comparison between Nutric Score and modified nutric score to assess ICU mortality in critically ill patients with COVID-19.Clin Nutr ESPEN. 2021 Aug;44:479-482. doi: 10.1016/j.clnesp.2021.04.026. Epub 2021 May 7. Clin Nutr ESPEN. 2021. PMID: 34330511 Free PMC article.
-
Nutritional risk in critically ill patients: how it is assessed, its prevalence and prognostic value: a systematic review.Nutr Rev. 2020 Dec 1;78(12):1052-1068. doi: 10.1093/nutrit/nuaa031. Nutr Rev. 2020. PMID: 32529226
-
Importance of nutritional assessment tools in the critically ill patient: A systematic review.Front Nutr. 2023 Jan 30;9:1073782. doi: 10.3389/fnut.2022.1073782. eCollection 2022. Front Nutr. 2023. PMID: 36793999 Free PMC article.
Cited by
-
The Utility of Muscle Ultrasound as a Predictor of Outcome in Guillain-Barré Syndrome Patients in the Intensive Care Unit: A Prospective Cohort Study.Indian J Crit Care Med. 2025 Mar;29(3):262-267. doi: 10.5005/jp-journals-10071-24928. Epub 2025 Feb 28. Indian J Crit Care Med. 2025. PMID: 40110240 Free PMC article.
-
Nutritional Biomarker-Guided Prediction of Postoperative Pain Outcomes in Elderly Patients Using a Shapley Additive Explanations (SHAP)-Informed XGBoost Approach.Cureus. 2025 May 29;17(5):e85048. doi: 10.7759/cureus.85048. eCollection 2025 May. Cureus. 2025. PMID: 40585729 Free PMC article.
-
Prognostic values of modified NUTRIC score to assess outcomes in critically ill patients admitted to the intensive care units: prospective observational study.BMC Anesthesiol. 2023 Apr 20;23(1):131. doi: 10.1186/s12871-023-02086-0. BMC Anesthesiol. 2023. PMID: 37081414 Free PMC article.
-
Risk of Malnutrition in Hospitalized COVID-19 Patients: A Systematic Review and Meta-Analysis.Nutrients. 2022 Dec 10;14(24):5267. doi: 10.3390/nu14245267. Nutrients. 2022. PMID: 36558436 Free PMC article.
-
Association between nutritional status, daily nutrition delivery and clinical outcomes of critically ill adult patients admitted to the intensive care unit: a protocol for Isfahan multicentre prospective observational cohort ICU study (the Isfahan-ICU study).BMJ Open. 2025 Jan 22;15(1):e090825. doi: 10.1136/bmjopen-2024-090825. BMJ Open. 2025. PMID: 39843374 Free PMC article.
References
-
- Alberda C., Gramlich L., Jones N., Jeejeebhoy K., Day A.G., Dhaliwal R., et al. The relationship between nutritional intake and clinical outcomes in critically ill patients: results of an international multicenter observational study. Intensive Care Med. 2009 Oct;35(10):1728–1737. doi: 10.1007/s00134-009-1567-4. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
