

Diagnostic, prognostic and differential-diagnostic relevance of pulmonary haemodynamic parameters during exercise: a systematic review
- PMID: 35332069
- PMCID: PMC9556812
- DOI: 10.1183/13993003.03181-2021
Diagnostic, prognostic and differential-diagnostic relevance of pulmonary haemodynamic parameters during exercise: a systematic review
Abstract
Background: The cardiopulmonary haemodynamic profile observed during exercise may identify patients with early-stage pulmonary vascular and primary cardiac diseases, and is used clinically to inform prognosis. However, a standardised approach to interpreting haemodynamic parameters is lacking.
Methods: We performed a systematic literature search according to PRISMA guidelines to identify parameters that may be diagnostic for an abnormal haemodynamic response to exercise and offer optimal prognostic and differential-diagnostic value. We performed random-effects meta-analyses of the normal values and report effect sizes as weighted mean±sd. Results of diagnostic and prognostic studies are reported descriptively.
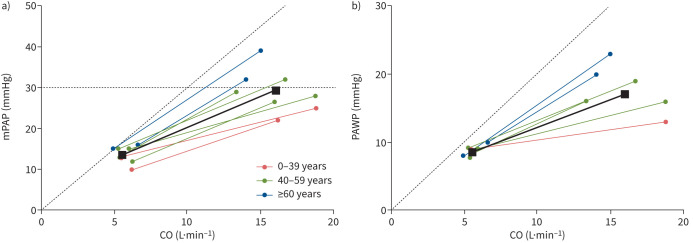
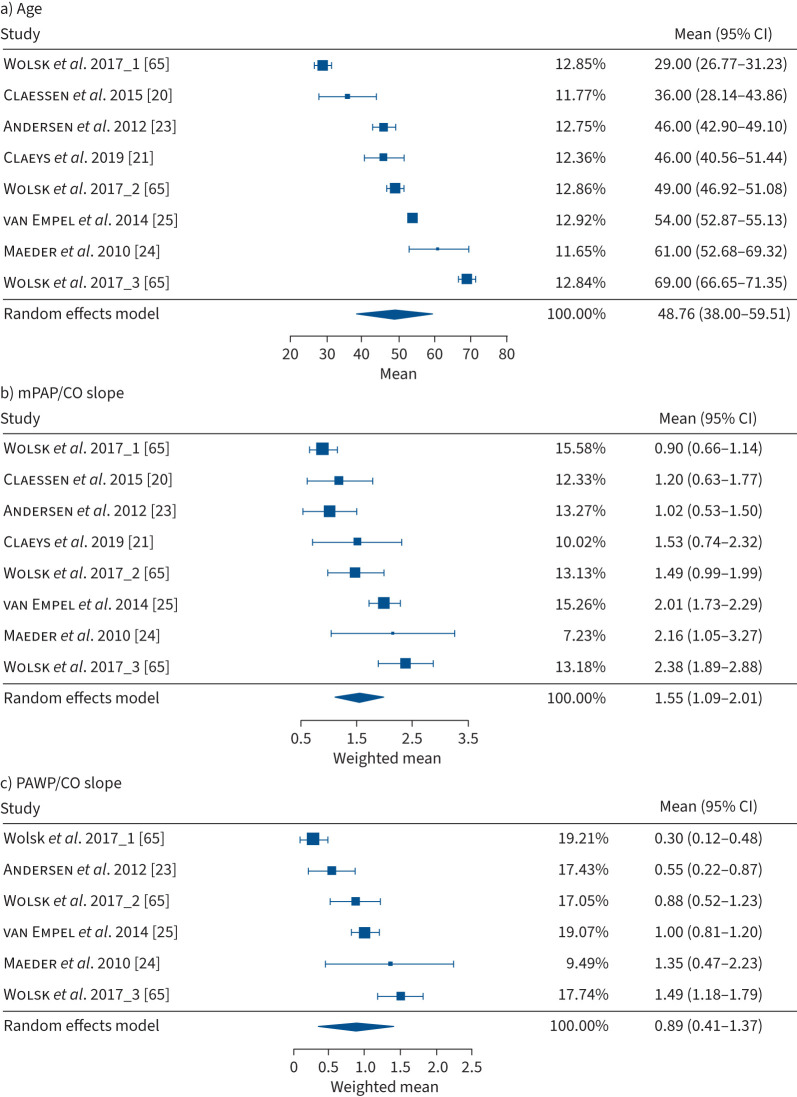
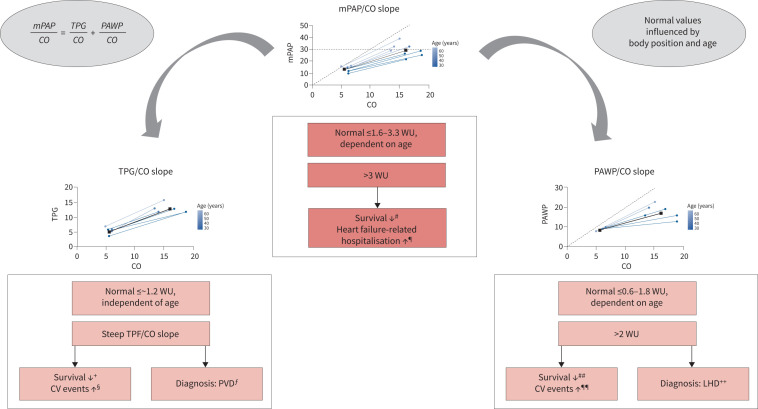
Results: We identified 45 eligible studies with a total of 5598 subjects. The mean pulmonary arterial pressure (mPAP)/cardiac output (CO) slope, pulmonary arterial wedge pressure (PAWP)/CO slope and peak cardiac index (or CO) provided the most consistent prognostic haemodynamic parameters during exercise. The best cut-offs for survival and cardiovascular events were a mPAP/CO slope >3 Wood units (WU) and PAWP/CO slope >2 WU. A PAWP/CO slope cut-off >2 WU best differentiated pre- from post-capillary causes of PAP elevation during exercise. Upper limits of normal (defined as mean+2sd) for the mPAP/CO and PAWP/CO slopes were strongly age-dependent and ranged in 30-70-year-old healthy subjects from 1.6 to 3.3 WU and 0.6 to 1.8 WU, respectively.
Conclusion: An increased mPAP/CO slope during exercise is associated with impaired survival and an independent, prognostically relevant cut-off >3 WU has been validated. A PAWP/CO slope >2 WU may be suitable for the differentiation between pre- and post-capillary causes of PAP increase during exercise.
The content of this work is not subject to copyright. Design and branding are copyright ©ERS 2022.
Conflict of interest statement
Conflict of interest: K. Zeder reports payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Janssen, and support for attending meetings and/or travel from MSD and Ferrer. B.A. Maron reports grants from Actelion Pharmaceuticals, Tenax Therapeutics, Regeneron Pharmaceuticals, Deerfield Corporation and NIH Research, and discloses the following patents: U.S. Patent #9,605,047, PCT/US2020/066886, PCT/US2019/059890 and PCT/US2015/029672. A. Berghold reports participation on a data safety monitoring board or advisory board for Roche. H. Olschewski reports consulting fees from Actelion, Chiesi, AstraZeneca, GSK, Bayer, Inventiva, Boehringer, Ferrer, Janssen, Menarini, MSD and Novartis, payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Springer and Medupdate, support for attending meetings and/or travel from Boehringer and Menarini, participation on a data safety monitoring board or advisory board for Aerovate, Bayer and Pfizer, receipt of equipment, materials, drugs, medical writing, gifts or other services from Algorithm Sciences, Boehringer and Inventiva, and is Deputy Director of the Ludwig Boltzmann Institute for Lung Vascular Research, Graz. The remaining authors disclose no potential conflicts of interest.
Figures
References
-
- World Health Organization Expert Committee on Chronic Cor Pulmonale . Chronic Cor Pulmonale: Report of an Expert Committee [meeting held in Geneva from 10 to 15 October 1960]. 1961. Available from: https://apps.who.int/iris/handle/10665/40483
-
- Hatano S, Strasser T, World Health Organization . Primary Pulmonary Hypertension: Report on a WHO Meeting, Geneva, 15–17 October 1973. 1975. Available from: https://apps.who.int/iris/handle/10665/39094
-
- Galiè N, Torbicki A, Barst R, et al. Guidelines on diagnosis and treatment of pulmonary arterial hypertension: The Task Force on Diagnosis and Treatment of Pulmonary Arterial Hypertension of the European Society of Cardiology. Eur Heart J 2004; 25: 2243–2278. doi: 10.1016/j.ehj.2004.09.014 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials