

A portrait of obstructive sleep apnea risk factors in 27,210 middle-aged and older adults in the Canadian Longitudinal Study on Aging
- PMID: 35332170
- PMCID: PMC8948183
- DOI: 10.1038/s41598-022-08164-6
A portrait of obstructive sleep apnea risk factors in 27,210 middle-aged and older adults in the Canadian Longitudinal Study on Aging
Abstract
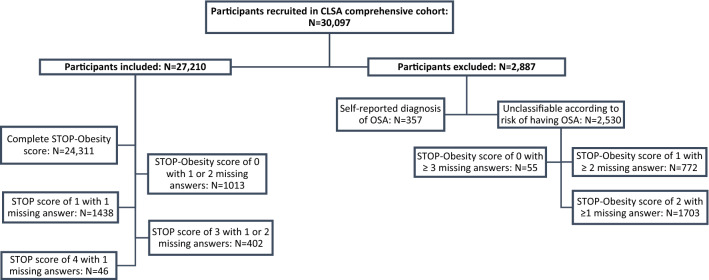
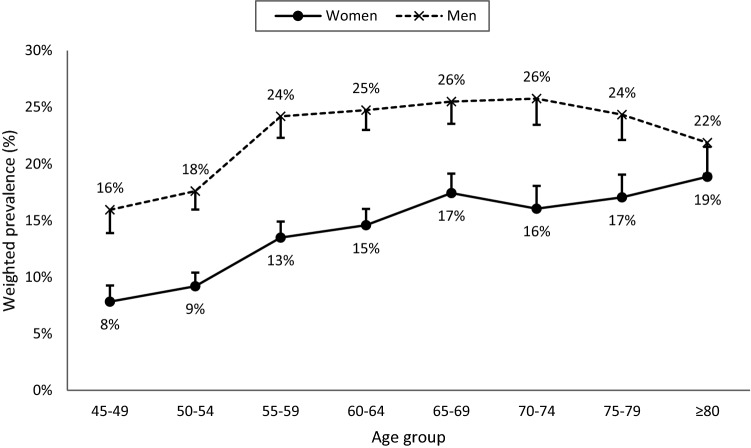
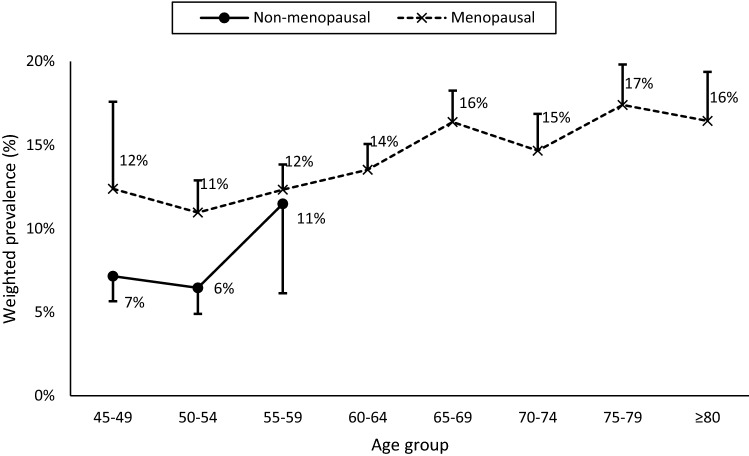
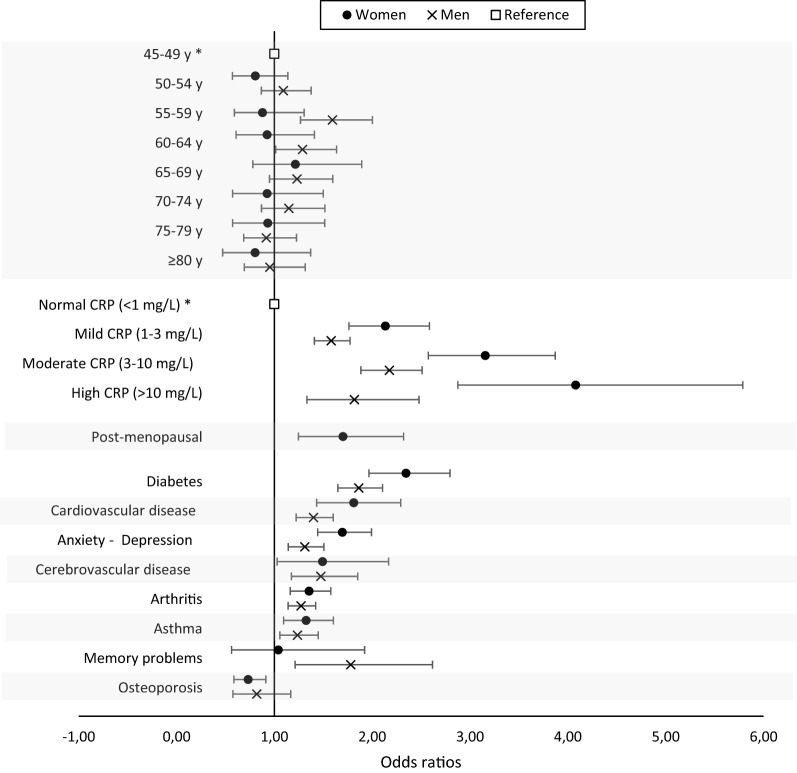
Determining the prevalence and characteristics of individuals susceptible to present with obstructive sleep apnea (OSA) is essential for developing targeted and efficient prevention and screening strategies. We included 27,210 participants aged ≥45 years old (50.3% women) from the Canadian Longitudinal Study on Aging. Using the STOP questionnaire combined to the percentage of body fat (%BF), we estimated the prevalence of individuals at high-risk for OSA in a sex and age-specific manner, and tested the relation with comorbidities, menopause and systemic inflammation. The prevalence was 17.5%, and was lower in women (13.1%) than in men (21.9%). A high level of high-sensitivity C-reactive protein was the strongest factor associated with OSA risk and this association was 1.3-2.3 times higher in women than in men. OSA risk increased with age, cardiovascular diseases, diabetes mellitus, anxio-depressive symptoms, asthma and arthritis. In women, post-menopausal status was associated with a high OSA risk. Nearly 1 adult out of 5 older than 45 is at risk for OSA in Canada. Comorbidities, menopause and systemic inflammation, more than age, explain increased OSA prevalence. Considering this high prevalence and associations with medical and mental comorbidities, health care practitioners should incorporate systematic OSA screening in their clinical procedures.
© 2022. The Author(s).
Conflict of interest statement
NG is supported by the Canadian Institutes of Health Research (CIHR) through a Foundation grant (#FDN154291), which funded the salary of CT, and studentships to MEMD and JL. NG, TDV, GM and JC receive salary awards from the Fonds de la recherche du Québec (FRQ). NC is supported by a fellowship from the FRQ-Santé. GE was supported by the Wilfred and Joyce Posluns Chair in Women’s Brain Health and Aging. This study was an initiative of the Canadian Sleep and Circadian Network, a network funded by the CIHR. The funding sources had no role in study design, data collection, analyses, interpretation, or writing of the manuscript. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Figures
Similar articles
-
Age- and sex-specific associations between obstructive sleep apnea risk and cognitive decline in middle-aged and older adults: A 3-year longitudinal analysis of the Canadian longitudinal study on aging.Sleep Med. 2023 Dec;112:77-87. doi: 10.1016/j.sleep.2023.09.029. Epub 2023 Oct 4. Sleep Med. 2023. PMID: 37832163
-
Association between risk of obstructive sleep apnea, inflammation and cognition after 45 years old in the Canadian Longitudinal Study on Aging.Sleep Med. 2022 Mar;91:21-30. doi: 10.1016/j.sleep.2022.02.006. Epub 2022 Feb 16. Sleep Med. 2022. PMID: 35245788
-
The prevalence and comorbidities of obstructive sleep apnea in middle-aged men and women: the Busselton Healthy Ageing Study.J Clin Sleep Med. 2021 Oct 1;17(10):2029-2039. doi: 10.5664/jcsm.9378. J Clin Sleep Med. 2021. PMID: 34606440 Free PMC article.
-
Obstructive sleep apnea in adults: epidemiology, clinical presentation, and treatment options.Adv Cardiol. 2011;46:1-42. doi: 10.1159/000327660. Epub 2011 Oct 13. Adv Cardiol. 2011. PMID: 22005188 Review.
-
Obstructive Sleep Apnea and Cardiovascular Disease: A Scientific Statement From the American Heart Association.Circulation. 2021 Jul 20;144(3):e56-e67. doi: 10.1161/CIR.0000000000000988. Epub 2021 Jun 21. Circulation. 2021. PMID: 34148375 Review.
Cited by
-
Delayed medical consultation and influencing factors in elderly patients with obstructive sleep apnea syndrome.Front Med (Lausanne). 2025 Jul 3;12:1555926. doi: 10.3389/fmed.2025.1555926. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40678127 Free PMC article.
-
Improving the cardiovascular outcomes of obstructive sleep apnea: Towards more precise hypoxia-based models of disease severity.Curr Sleep Med Rep. 2025;11(1):3. doi: 10.1007/s40675-024-00315-7. Epub 2025 Jan 3. Curr Sleep Med Rep. 2025. PMID: 40416582
-
Cardiovascular Disease Outcomes Associated with Obstructive Sleep Apnea in Diabetics: A Systematic Review and Meta-Analysis.Diseases. 2023 Aug 7;11(3):103. doi: 10.3390/diseases11030103. Diseases. 2023. PMID: 37606474 Free PMC article. Review.
-
Assessment of obstructive sleep apnea rate and associated factors among Lebanese adults: a cross-sectional study.Front Public Health. 2025 Feb 13;13:1443920. doi: 10.3389/fpubh.2025.1443920. eCollection 2025. Front Public Health. 2025. PMID: 40017556 Free PMC article.
-
Prevalence and factors associated with high risk for obstructive sleep apnea in schizophrenia spectrum disorder patients on long-term clozapine.Indian J Psychiatry. 2024 Dec;66(12):1159-1164. doi: 10.4103/indianjpsychiatry.indianjpsychiatry_544_24. Epub 2024 Dec 12. Indian J Psychiatry. 2024. PMID: 39867240 Free PMC article.
References
-
- Benjafield, A. et al. Global prevalence of obstructive sleep apnea in adults. Am. J. Respir. Crit. Care Med.American T, A3962–A3962 (2018).
-
- Carter R, Watenpaugh DE. Obesity and obstructive sleep apnea: or is it OSA and obesity? Pathophysiology. 2008;15:71–77. - PubMed
-
- McNicholas, W. T., Bonsignore, M. R. & The Management Committee of EU COST ACTION B26. Sleep Apnoea as an Independent Risk for Cardiovascular Disease: Current Evidence, Basic Mechanisms and Research Priorities. Eur. Respir. J.29, 156–178 (2007) - PubMed
-
- Edwards C, Almeida OP, Ford AH. Obstructive sleep apnea and depression: a systematic review and meta-analysis. Maturitas. 2020;142:45–54. - PubMed
-
- Yeghiazarians Y, et al. Obstructive sleep apnea and cardiovascular disease: a scientific statement from the american heart association. Circulation. 2021;144:e56–e67. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
