

Immune responses against SARS-CoV-2 variants after two and three doses of vaccine in B-cell malignancies: UK PROSECO study
- PMID: 35332334
- PMCID: PMC9135622
- DOI: 10.1038/s43018-022-00364-3
Immune responses against SARS-CoV-2 variants after two and three doses of vaccine in B-cell malignancies: UK PROSECO study
Abstract
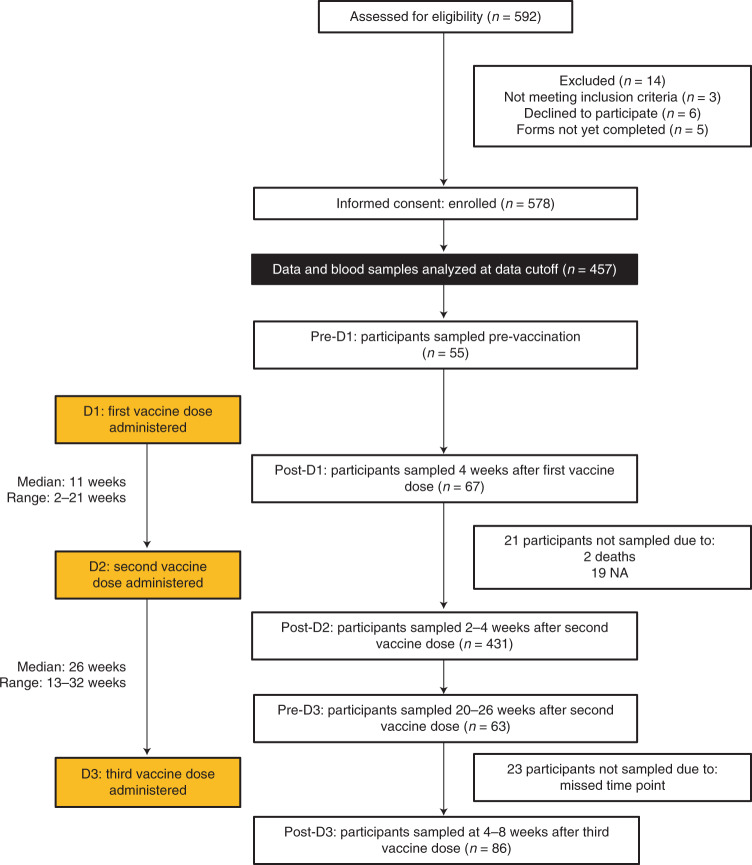
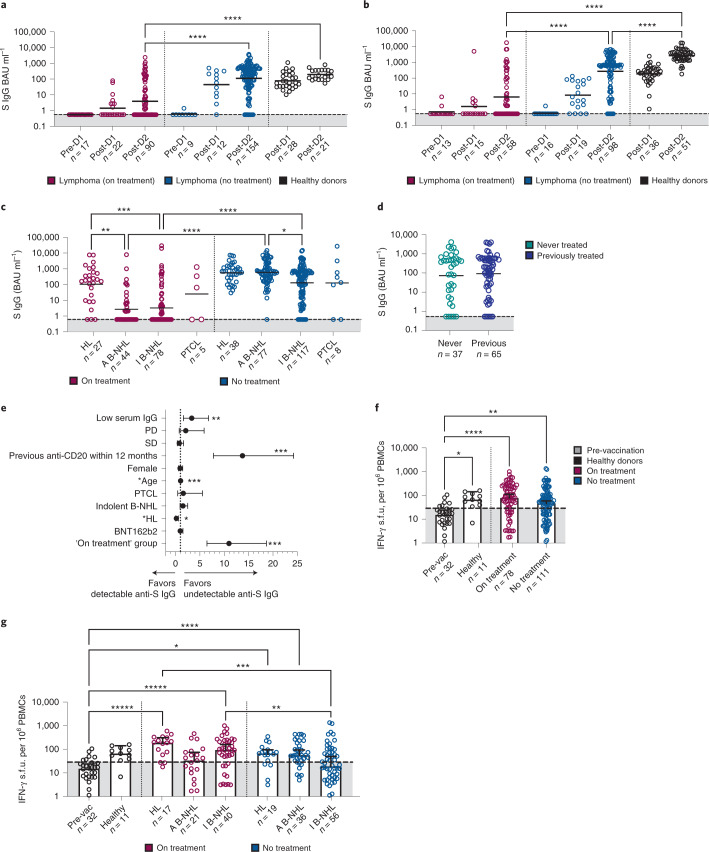
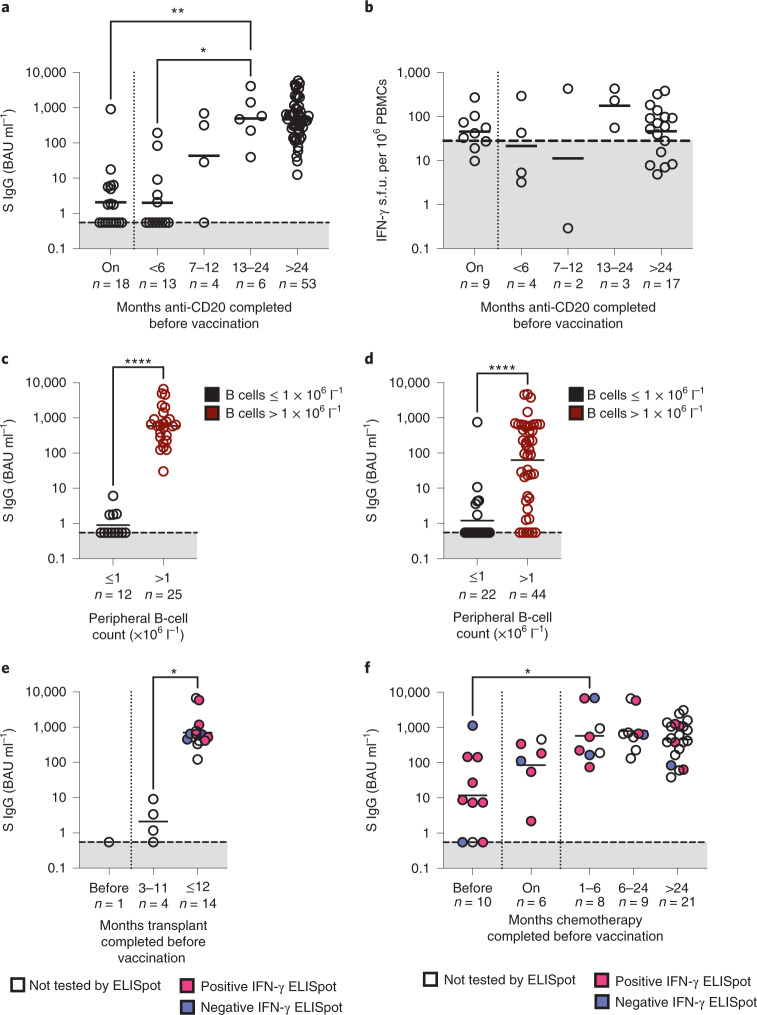
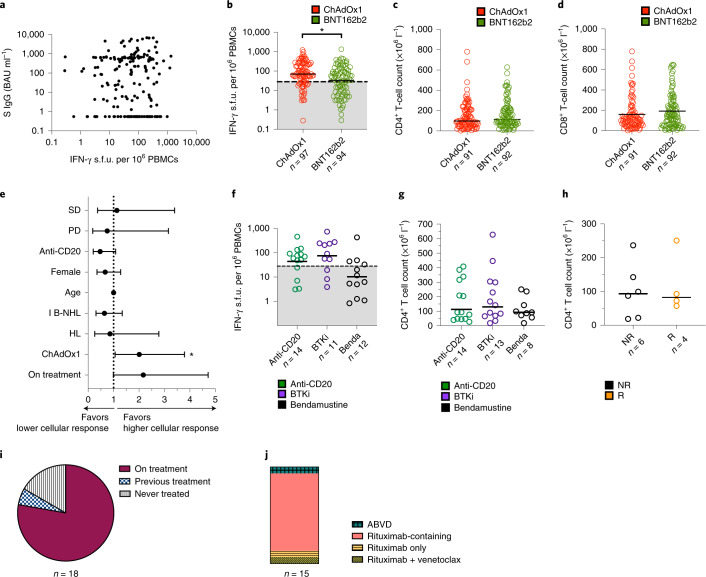
Patients with hematological malignancies are at increased risk of severe COVID-19 outcomes due to compromised immune responses, but the insights of these studies have been compromised due to intrinsic limitations in study design. Here we present the PROSECO prospective observational study ( NCT04858568 ) on 457 patients with lymphoma that received two or three COVID-19 vaccine doses. We show undetectable humoral responses following two vaccine doses in 52% of patients undergoing active anticancer treatment. Moreover, 60% of patients on anti-CD20 therapy had undetectable antibodies following full vaccination within 12 months of receiving their anticancer therapy. However, 70% of individuals with indolent B-cell lymphoma displayed improved antibody responses following booster vaccination. Notably, 63% of all patients displayed antigen-specific T-cell responses, which increased after a third dose irrespective of their cancer treatment status. Our results emphasize the urgency of careful monitoring of COVID-19-specific immune responses to guide vaccination schemes in these vulnerable populations.
© 2022. The Author(s).
Conflict of interest statement
S.H.L., N.C., M.J., D.J.P., A.O., H.C., C.M., A.K., A.R.C., A.H.T., K.L., D.J., B.W., T.W., A.T.B., K.R., B.S., C.G., D.A., J.F., O.B., J.B., V.M., A.B.A.-N., L.R., T.M., P.W.M.J. and D.G. declare no competing interests. C.F. receives consultancy fees from AstraZeneca and participates in an advisory board for AstraZeneca. M.A. receives research funding from Pfizer. G.P.C. receives research funding from Pfizer and participates in advisory boards for AstraZeneca and Pfizer. R.L. reports receiving speaker fees and honoraria from Janssen. A.J.D. reports receiving research funding and honoraria from AstraZeneca and Janssen. S.N.F. participates in advisory boards related to vaccines or grants for contract commercial clinical trials that were paid to S.N.F.’s institution (with no personal payment of any kind) from AstraZeneca/Medimmune, Sanofi, Pfizer, Seqirus, Merck, GSK, J&J, Merck and Valneva, outside the submitted work.
Figures


Comment in
-
A needed boost against COVID-19 in lymphoma.Nat Cancer. 2022 May;3(5):526-527. doi: 10.1038/s43018-022-00374-1. Nat Cancer. 2022. PMID: 35624336 No abstract available.
References
Publication types
MeSH terms
Substances
Supplementary concepts
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
