

Assessment of neonatal respiratory rate variability
- PMID: 35332406
- PMCID: PMC9637627
- DOI: 10.1007/s10877-022-00840-2
Assessment of neonatal respiratory rate variability
Abstract
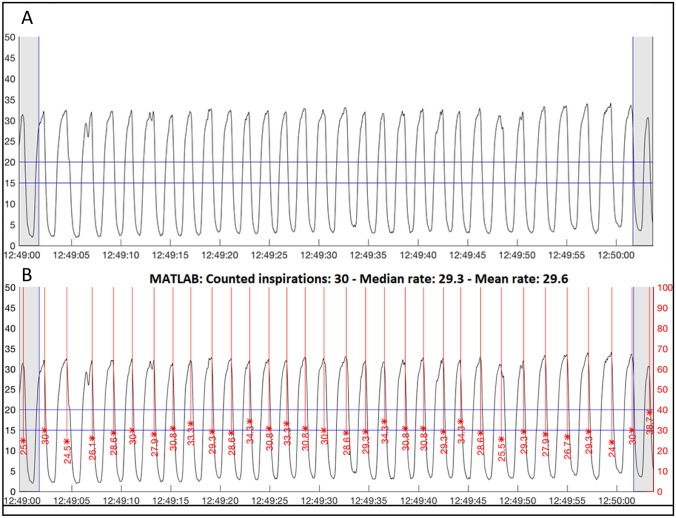
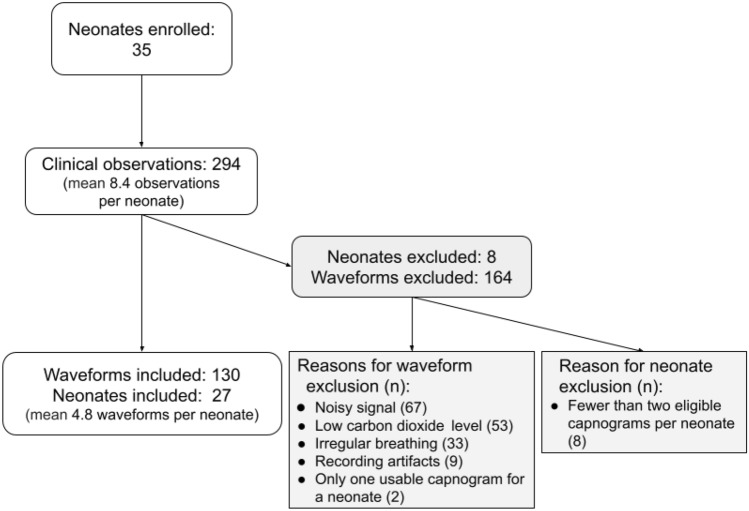
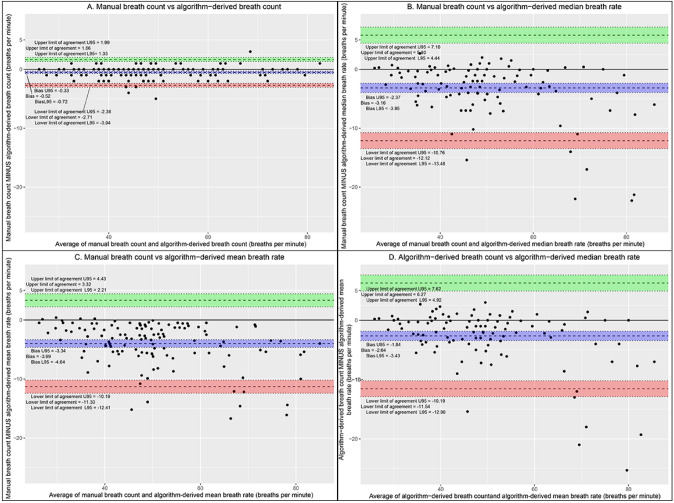
Accurate measurement of respiratory rate (RR) in neonates is challenging due to high neonatal RR variability (RRV). There is growing evidence that RRV measurement could inform and guide neonatal care. We sought to quantify neonatal RRV during a clinical study in which we compared multiparameter continuous physiological monitoring (MCPM) devices. Measurements of capnography-recorded exhaled carbon dioxide across 60-s epochs were collected from neonates admitted to the neonatal unit at Aga Khan University-Nairobi hospital. Breaths were manually counted from capnograms and using an automated signal detection algorithm which also calculated mean and median RR for each epoch. Outcome measures were between- and within-neonate RRV, between- and within-epoch RRV, and 95% limits of agreement, bias, and root-mean-square deviation. Twenty-seven neonates were included, with 130 epochs analysed. Mean manual breath count (MBC) was 48 breaths per minute. Median RRV ranged from 11.5% (interquartile range (IQR) 6.8-18.9%) to 28.1% (IQR 23.5-36.7%). Bias and limits of agreement for MBC vs algorithm-derived breath count, MBC vs algorithm-derived median breath rate, MBC vs algorithm-derived mean breath rate were - 0.5 (- 2.7, 1.66), - 3.16 (- 12.12, 5.8), and - 3.99 (- 11.3, 3.32), respectively. The marked RRV highlights the challenge of performing accurate RR measurements in neonates. More research is required to optimize the use of RRV to improve care. When evaluating MCPM devices, accuracy thresholds should be less stringent in newborns due to increased RRV. Lastly, median RR, which discounts the impact of extreme outliers, may be more reflective of the underlying physiological control of breathing.
Keywords: Child health; Critical care; Delivery of health care; Diagnosis; Patient care.
© 2022. The Author(s).
Conflict of interest statement
All authors declare no competing interests.
Figures

References
-
- World Health Organization. Integrated management of childhood illness: caring for newborns and children in the community; 2011.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
