

Waveform Morphology as a Surrogate for ICP Monitoring: A Comparison Between an Invasive and a Noninvasive Method
- PMID: 35332426
- PMCID: PMC8947812
- DOI: 10.1007/s12028-022-01477-4
Waveform Morphology as a Surrogate for ICP Monitoring: A Comparison Between an Invasive and a Noninvasive Method
Abstract
Background: Although the placement of an intraventricular catheter remains the gold standard technique for measuring intracranial pressure (ICP), the method has several limitations. Therefore, noninvasive alternatives to ICP (ICPni) measurement are of great interest. The main objective of this study was to compare the correlation and agreement of wave morphology between ICP (standard intraventricular ICP monitoring) and a new ICPni monitor in patients admitted with stroke. The second objective was to estimate the discrimination of the noninvasive method to detect intracranial hypertension.
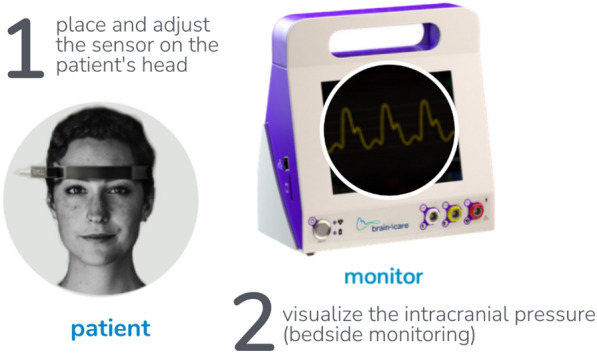
Methods: We prospectively collected data of adults admitted to an intensive care unit with subarachnoid hemorrhage, intracerebral hemorrhage, or ischemic stroke in whom an invasive ICP monitor was placed. Measurements were simultaneously collected from two parameters [time-to-peak (TTP) and the ratio regarding the second and first peak of the ICP wave (P2/P1 ratio)] of ICP and ICPni wave morphology monitors (Brain4care). Intracranial hypertension was defined as an invasively measured sustained ICP > 20 mm Hg for at least 5 min.
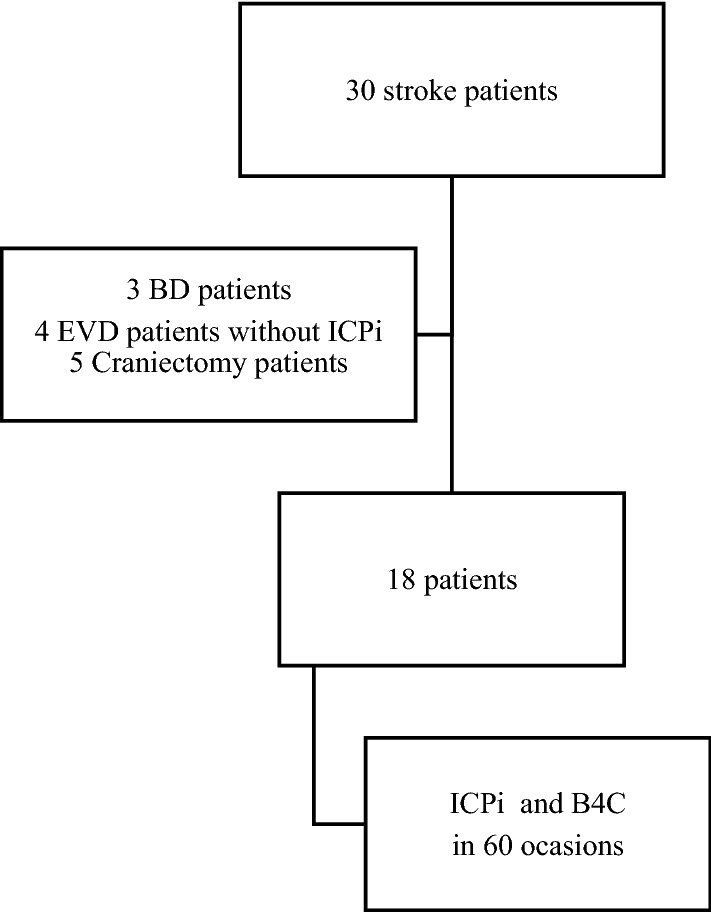
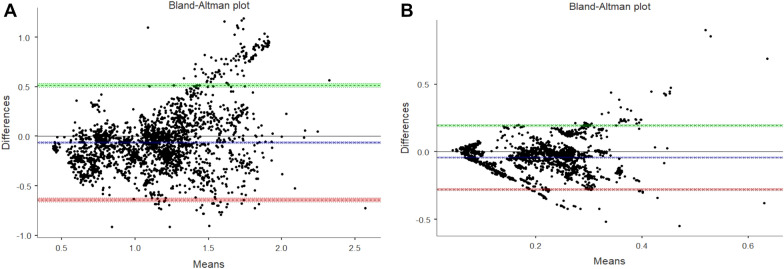
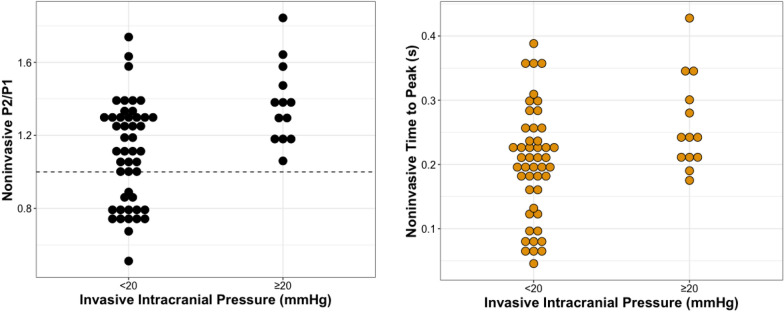
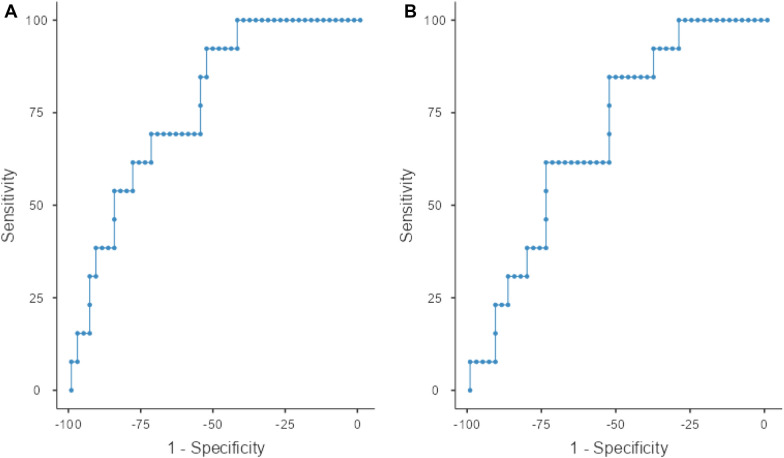
Results: We studied 18 patients (subarachnoid hemorrhage = 14; intracerebral hemorrhage = 3; ischemic stroke = 1) on 60 occasions with a median age of 52 ± 14.3 years. A total of 197,400 waves (2495 min) from both ICP (standard ICP monitoring) and the ICPni monitor were sliced into 1-min-long segments, and we determined TTP and the P2/P1 ratio from the mean pulse. The median invasively measured ICP was 13 (9.8-16.2) mm Hg, and intracranial hypertension was present on 18 occasions (30%). The correlation and agreement between invasive and noninvasive methods for wave morphology were strong for the P2/P1 ratio and moderate for TTP using categoric (κ agreement 88.1% and 71.3%, respectively) and continuous (intraclass correlation coefficient 0.831 and 0.584, respectively) measures. There was a moderate but significant correlation with the mean ICP value (P2/P1 ratio r = 0.427; TTP r = 0.353; p < 0.001 for all) between noninvasive and invasive techniques. The areas under the curve to estimate intracranial hypertension were 0.786 [95% confidence interval (CI) 0.72-0.93] for the P2/P1 ratio and 0.694 (95% CI 0.60-0.74) for TTP.
Conclusions: The new ICPni wave morphology monitor showed a good agreement with the standard invasive method and an acceptable discriminatory power to detect intracranial hypertension. Clinical trial registration Trial registration: NCT05121155.
Keywords: Brain trauma; Intracranial pressure wave morphology; Neurointensive care unit; Noninvasive intracranial pressure monitor; Stroke.
© 2022. Springer Science+Business Media, LLC, part of Springer Nature and Neurocritical Care Society.
Conflict of interest statement
None.
Figures
References
-
- Fried HI, Nathan BR, Rowe AS, Zabramski JM, Andaluz N, Bhimraj A, et al. The insertion and management of external ventricular drains: an evidence-based consensus statement: a statement for healthcare professionals from the neurocritical care society. Neurocrit Care. 2016;24(1):61–81. doi: 10.1007/s12028-015-0224-8. - DOI - PubMed
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
