

P Wave Parameters and Indices: A Critical Appraisal of Clinical Utility, Challenges, and Future Research-A Consensus Document Endorsed by the International Society of Electrocardiology and the International Society for Holter and Noninvasive Electrocardiology
- PMID: 35333097
- PMCID: PMC9070127
- DOI: 10.1161/CIRCEP.121.010435
P Wave Parameters and Indices: A Critical Appraisal of Clinical Utility, Challenges, and Future Research-A Consensus Document Endorsed by the International Society of Electrocardiology and the International Society for Holter and Noninvasive Electrocardiology
Abstract
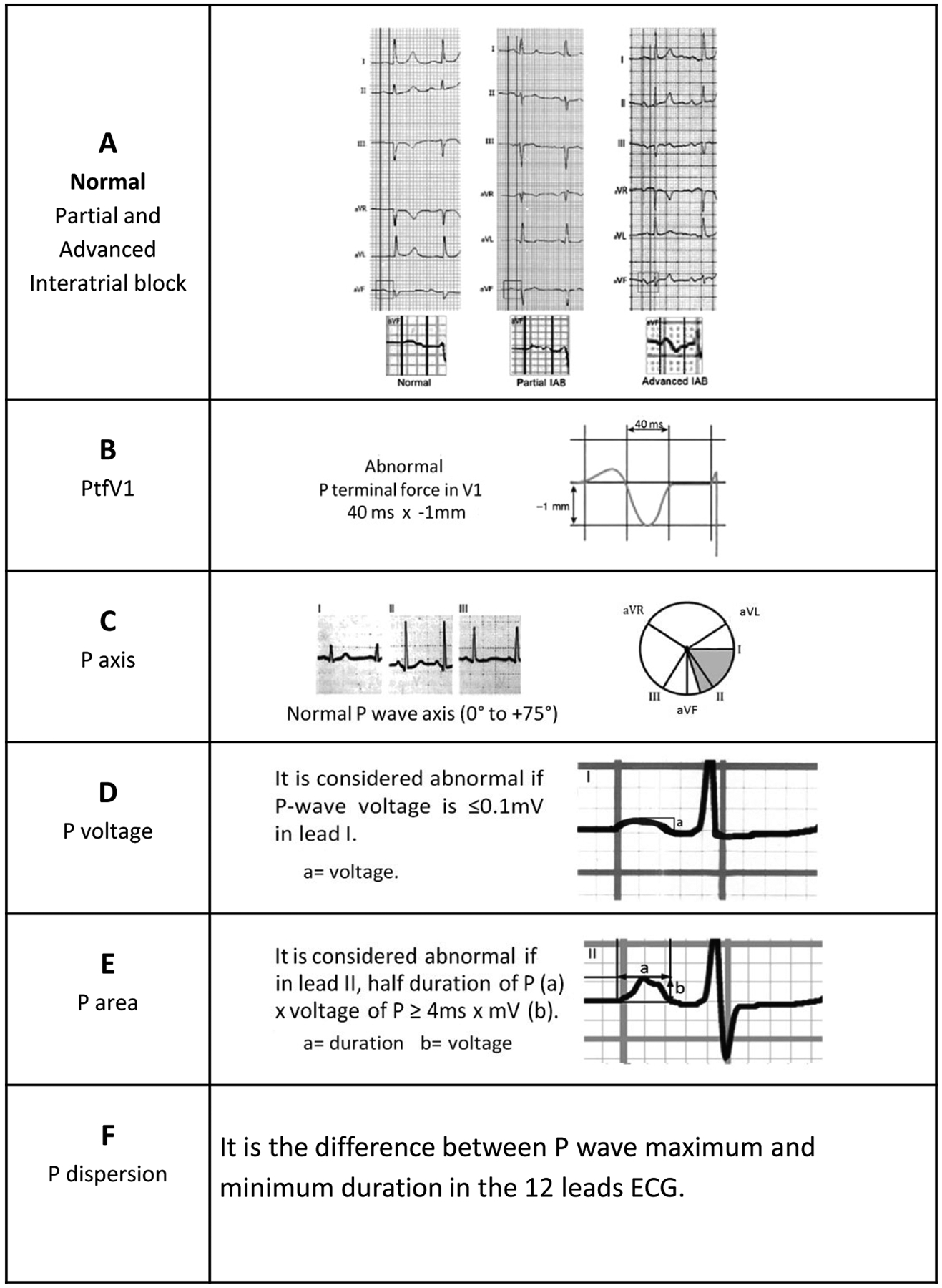
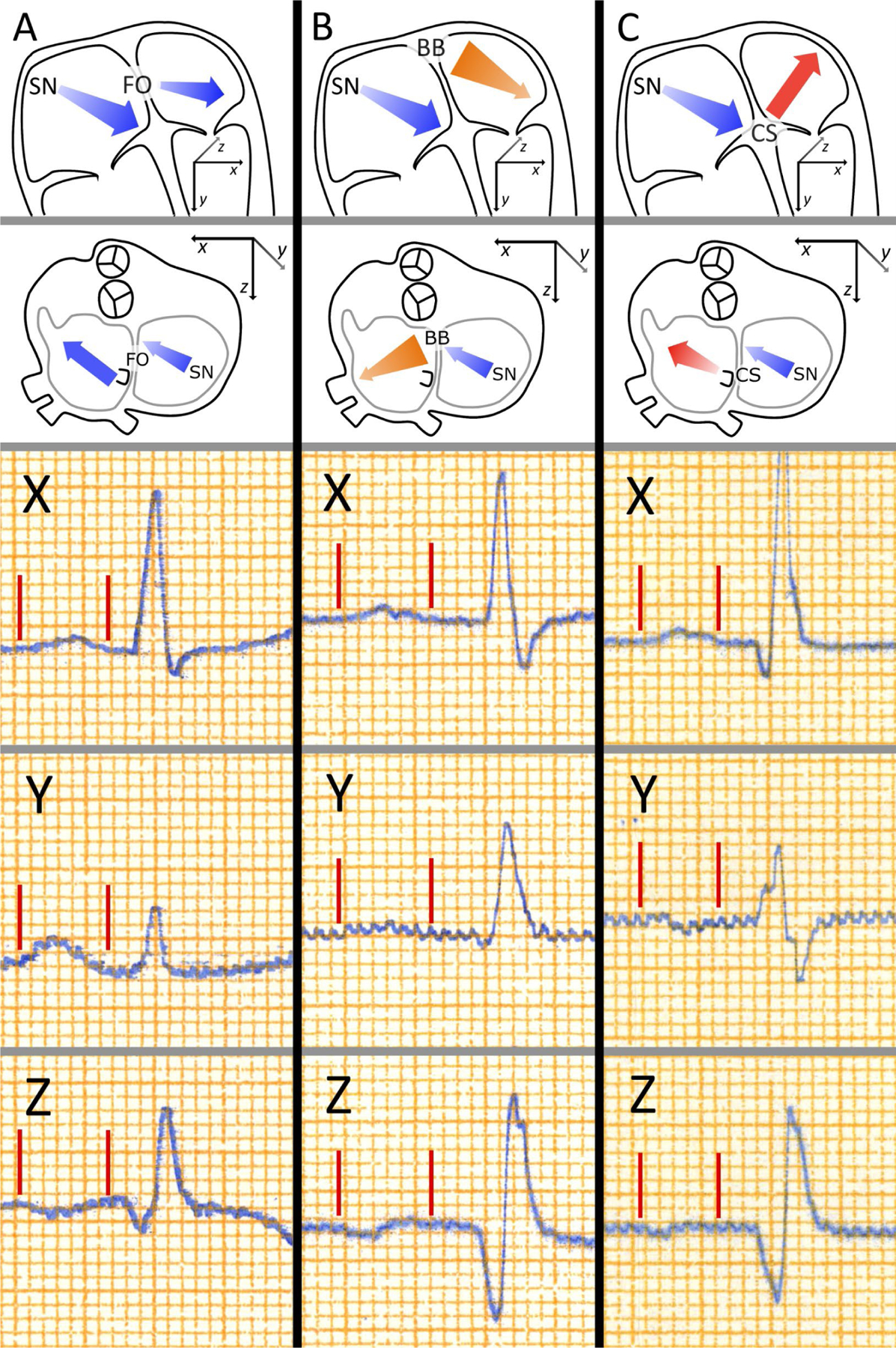
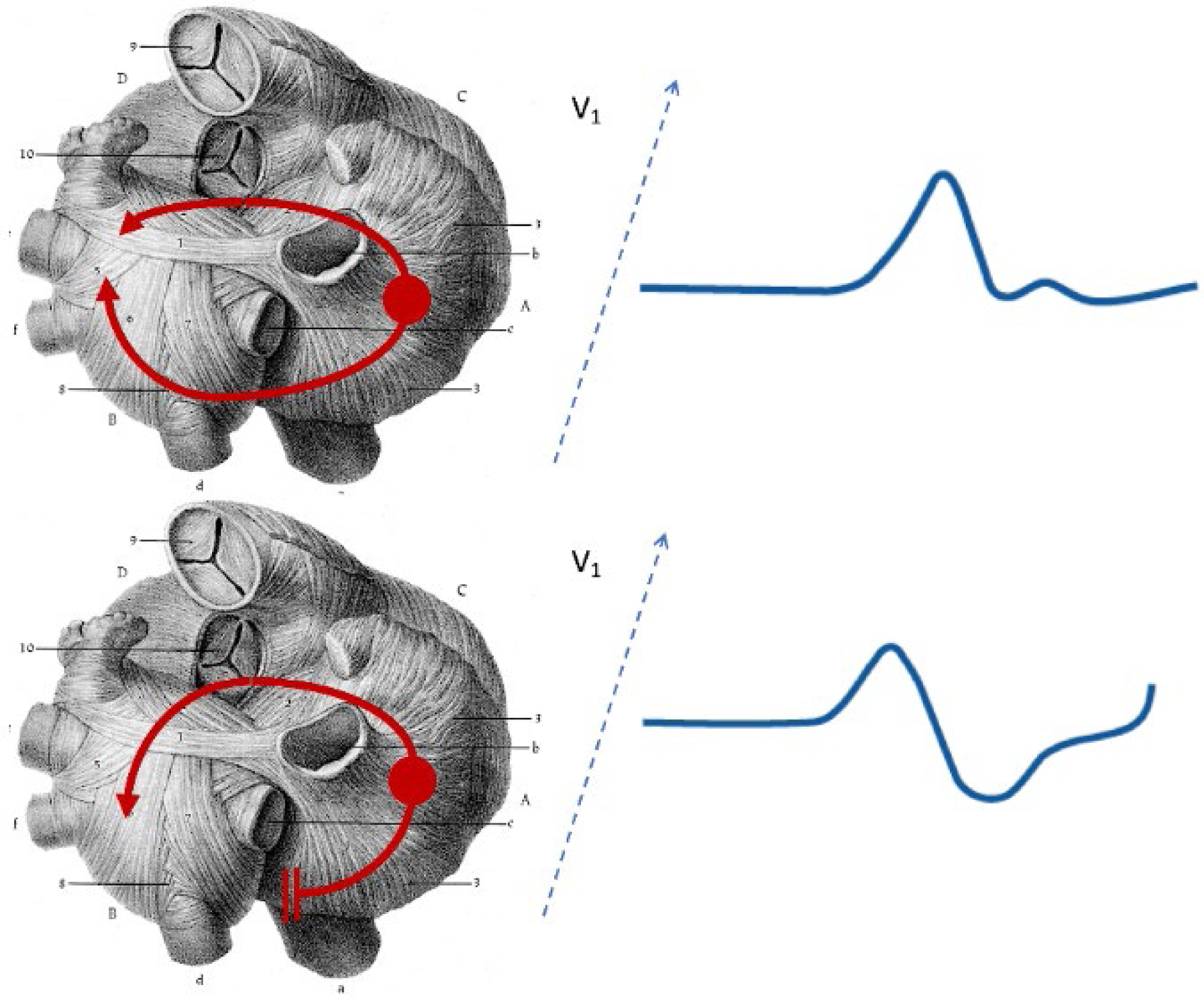
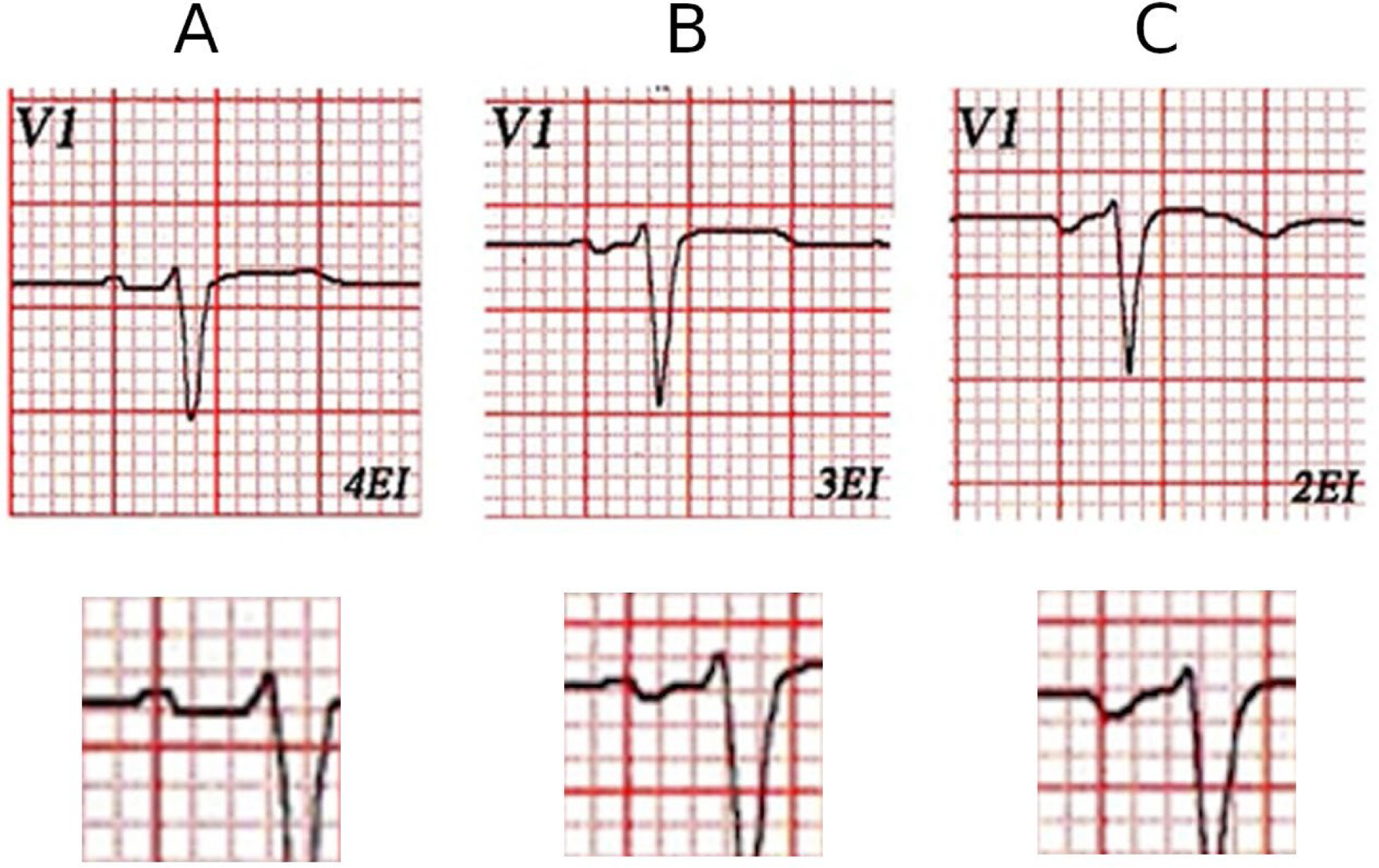
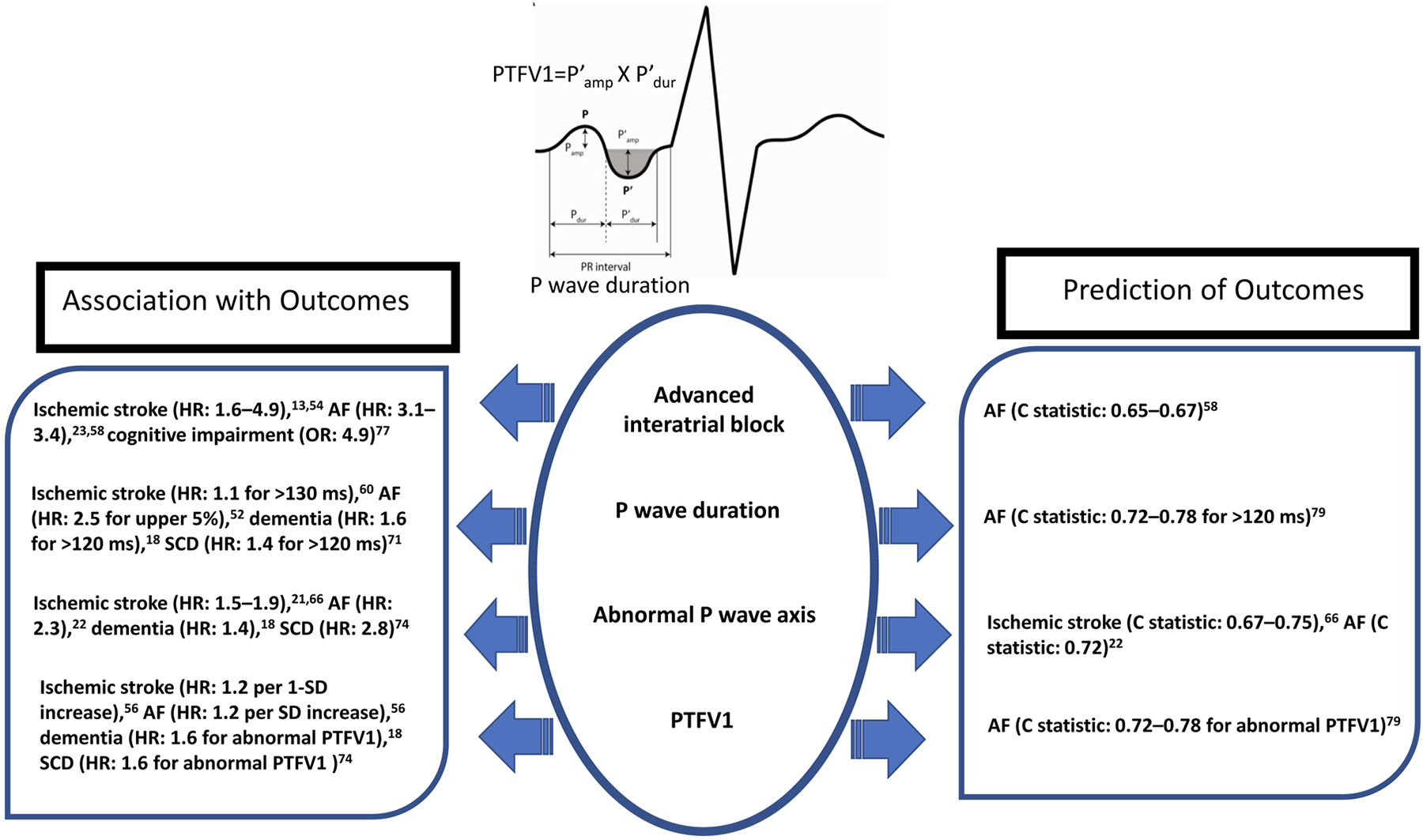
Atrial cardiomyopathy, characterized by abnormalities in atrial structure and function, is associated with increased risk of adverse cardiovascular and neurocognitive outcomes, independent of atrial fibrillation. There exists a critical unmet need for a clinical tool that is cost-effective, easy to use, and that can diagnose atrial cardiomyopathy. P wave parameters (PWPs) reflect underlying atrial structure, size, and electrical activation; alterations in these factors manifest as abnormalities in PWPs that can be readily ascertained from a standard 12-lead ECG and potentially be used to aid clinical decision-making. PWPs include P wave duration, interatrial block, P wave terminal force in V1, P wave axis, P wave voltage, P wave area, and P wave dispersion. PWPs can be combined to yield an index (P wave index), such as the morphology-voltage-P-wave duration ECG risk score. Abnormal PWPs have been shown in population-based cohort studies to be independently associated with higher risks of atrial fibrillation, ischemic stroke, sudden cardiac death, and dementia. Additionally, PWPs, either individually or in combination (as a P wave index), have been reported to enhance prediction of atrial fibrillation or ischemic stroke. To facilitate translation of PWPs to routine clinical practice, additional work is needed to standardize measurement of PWPs (eg, via semiautomated or automated measurement), confirm their reliability and predictive value, leverage novel approaches (eg, wavelet analysis of P waves and machine learning algorithms), and finally, define the risk-benefit ratio of specific interventions in high-risk individuals. Our ultimate goal is to repurpose the ubiquitous 12-lead ECG to advance the study, diagnosis, and treatment of atrial cardiomyopathy, thus overcoming critical challenges in prevention of cardiovascular disease and dementia.
Keywords: atrial fibrillation; cardiomyopathy; cardiovascular disease; interatrial block; ischemic stroke.
Figures
References
-
- Donal E, Lip GY, Galderisi M, Goette A, Shah D, Marwan M, Lederlin M, Mondillo S, Edvardsen T, Sitges M, et al. EACVI/EHRA Expert Consensus Document on the role of multi-modality imaging for the evaluation of patients with atrial fibrillation. Eur Heart J Cardiovasc Imaging. 2016;17:355–83. - PubMed
-
- Tiffany Win T, Ambale Venkatesh B, Volpe GJ, Mewton N, Rizzi P, Sharma RK, Strauss DG, Lima JA, Tereshchenko LG. Associations of electrocardiographic P-wave characteristics with left atrial function, and diffuse left ventricular fibrosis defined by cardiac magnetic resonance: The PRIMERI Study. Heart Rhythm. 2015;12:155–62. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
