

Predicting the likelihood of successful medical treatment of early pregnancy loss: development and internal validation of a clinical prediction model
- PMID: 35333346
- PMCID: PMC9071219
- DOI: 10.1093/humrep/deac048
Predicting the likelihood of successful medical treatment of early pregnancy loss: development and internal validation of a clinical prediction model
Abstract
Study question: What are clinical predictors for successful medical treatment in case of early pregnancy loss (EPL)?
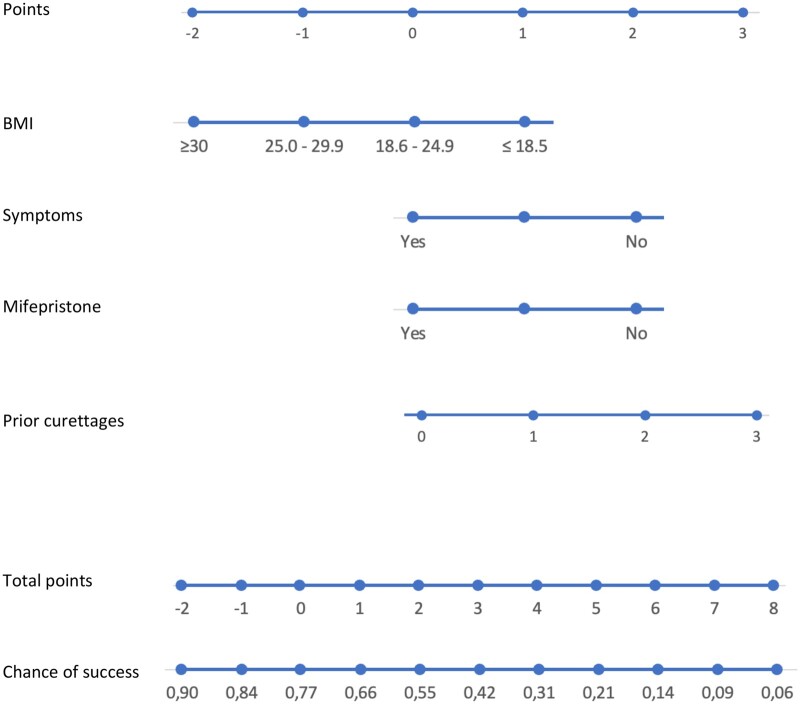
Summary answer: Use of mifepristone, BMI, number of previous uterine aspirations and the presence of minor clinical symptoms (slight vaginal bleeding or some abdominal cramps) at treatment start are predictors for successful medical treatment in case of EPL.
What is known already: Success rates of medical treatment for EPL vary strongly, between but also within different treatment regimens. Up until now, although some predictors have been identified, no clinical prediction model has been developed yet.
Study design, size, duration: Secondary analysis of a multicentre randomized controlled trial in 17 Dutch hospitals, executed between 28 June 2018 and 8 January 2020.
Participants/materials, setting, methods: Women with a non-viable pregnancy between 6 and 14 weeks of gestational age, who opted for medical treatment after a minimum of 1 week of unsuccessful expectant management. Potential predictors for successful medical treatment of EPL were chosen based on literature and expert opinions. We internally validated the prediction model using bootstrapping techniques.
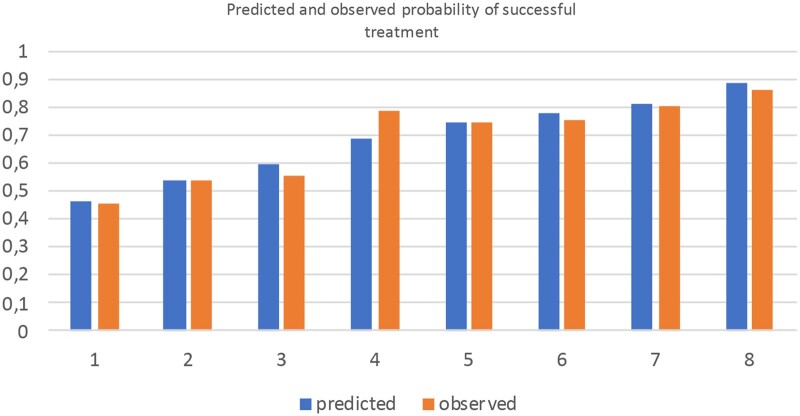
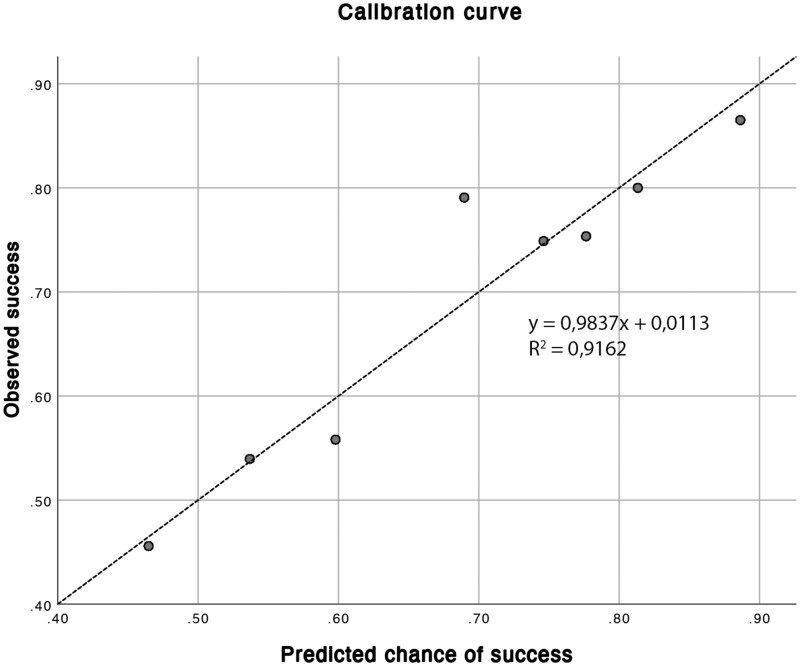
Main results and the role of chance: 237 out of 344 women had a successful medical EPL treatment (68.9%). The model includes the following variables: use of mifepristone, BMI, number of previous uterine aspirations and the presence of minor clinical symptoms (slight vaginal bleeding or some abdominal cramps) at treatment start. The model shows a moderate capacity to discriminate between success and failure of treatment, with an AUC of 67.6% (95% CI = 64.9-70.3%). The model had a good fit comparing predicted to observed probabilities of success but might underestimate treatment success in women with a predicted probability of success of ∼70%.
Limitations, reasons for caution: The vast majority (90.4%) of women were Caucasian, potentially leading to less optimal model performance in a non-Caucasian population. Limitations of our model are that we have not yet been able to externally validate its performance and clinical impact, and the moderate accuracy of the prediction model of 0.67.
Wider implications of the findings: We developed a prediction model, aimed to improve and personalize counselling for medical treatment of EPL by providing a woman with her individual chance of complete evacuation.
Study funding/competing interest(s): The Triple M Trial, upon which this secondary analysis was performed, was funded by the Healthcare Insurers Innovation Foundation (project number 3080 B15-191).
Trial registration number: Clinicaltrials.gov: NCT03212352.
Keywords: early pregnancy loss; mifepristone; misoprostol; personalized medicine; prediction model.
© The Author(s) 2022. Published by Oxford University Press on behalf of European Society of Human Reproduction and Embryology.
Figures
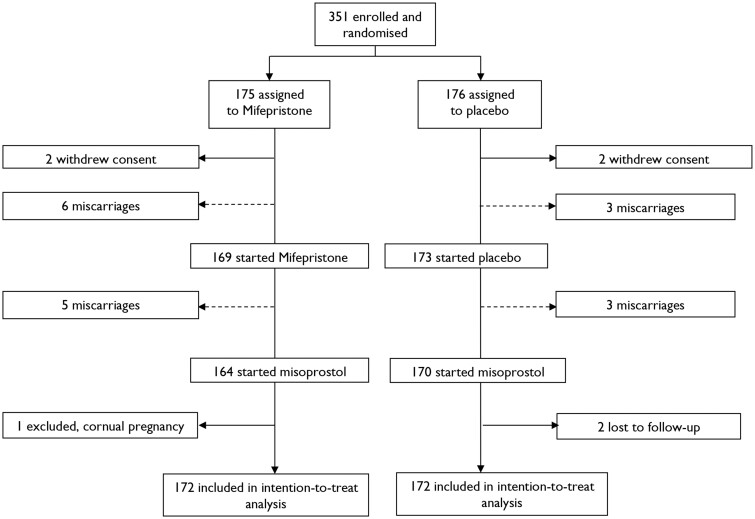
 = included in intention-to-treat analysis.
= included in intention-to-treat analysis.  = excluded from intention-to-treat analysis.
= excluded from intention-to-treat analysis.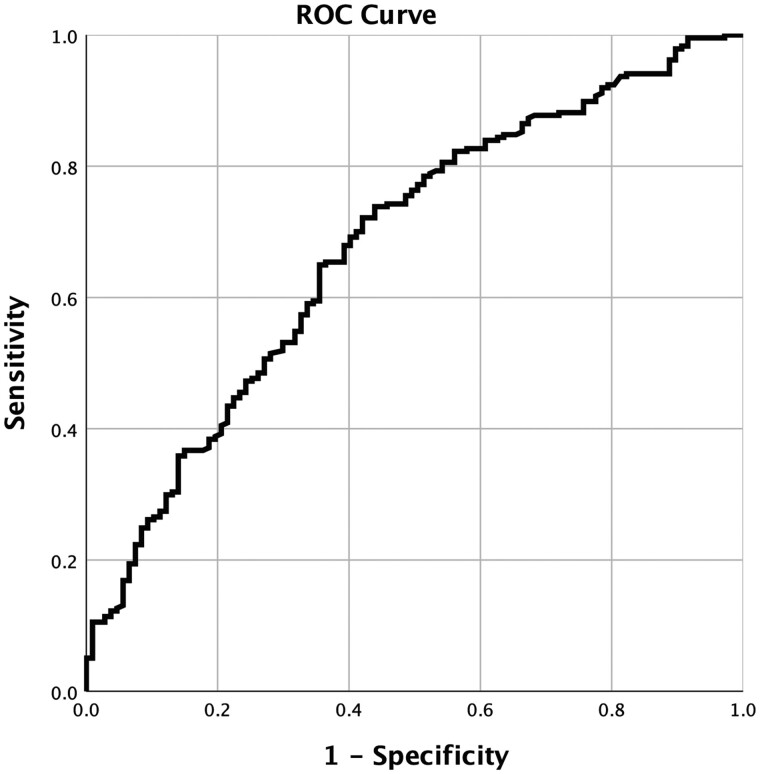
References
-
- ACOG: The American College of Obstetricians and Gynaecologists. Clinical management guidelines for obstetrician–gynecologists. Obstet Gynecol 2019;133:168–186.
-
- Ammon Avalos L, Galindo C, Li DK.. A systematic review to calculate background miscarriage rates using life table analysis. Birth Defects Res A Clin Mol Teratol 2012;94:417–423. - PubMed
-
- Ashok PW, Templeton A, Wagaarachchi PT, Flett GMM.. Factors affecting the outcome of early medical abortion: a review of 4132 consecutive cases. BJOG 2002;109:1281–1289. - PubMed
-
- Bartley J, Tong S, Everington D, Baird DT.. Parity is a major determinant of success rate in medical abortion: a retrospective analysis of 3161 consecutive cases of early medical abortion treated with reduced doses of mifepristone and vaginal gemeprost. Contraception 2000;62:297–303. - PubMed
-
- Broeze KA, Opmeer BC, Bachmann LM, Broekmans FJ, Bossuyt PMM, Coppus SFPJ, Johnson NP, Khan KS, Riet G, Van Der Veen F. et al. Methodology individual patient data meta-analysis of diagnostic and prognostic studies in obstetrics, gynaecology and reproductive medicine. BMC Med Res Methodol 2009;9:22. - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
