

Pembrolizumab Alone or With Chemotherapy for Recurrent/Metastatic Head and Neck Squamous Cell Carcinoma in KEYNOTE-048: Subgroup Analysis by Programmed Death Ligand-1 Combined Positive Score
- PMID: 35333599
- PMCID: PMC9287281
- DOI: 10.1200/JCO.21.02198
Pembrolizumab Alone or With Chemotherapy for Recurrent/Metastatic Head and Neck Squamous Cell Carcinoma in KEYNOTE-048: Subgroup Analysis by Programmed Death Ligand-1 Combined Positive Score
Abstract
Purpose: The phase III KEYNOTE-048 (ClinicalTrials.gov identifier: NCT02358031) trial of pembrolizumab in recurrent or metastatic (R/M) head and neck squamous cell carcinoma (HNSCC) included planned efficacy analyses in the total population and in participants with programmed death ligand-1 (PD-L1) combined positive score (CPS) ≥ 1 and CPS ≥ 20. To further characterize the predictive value of PD-L1 expression on outcome, we conducted efficacy analyses in the PD-L1 CPS < 1 and CPS 1-19 subgroups in KEYNOTE-048.
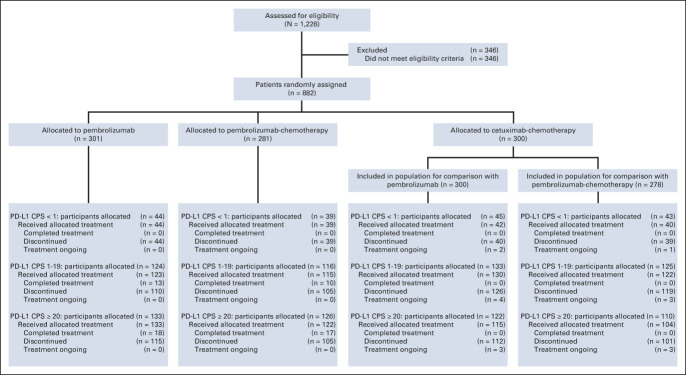
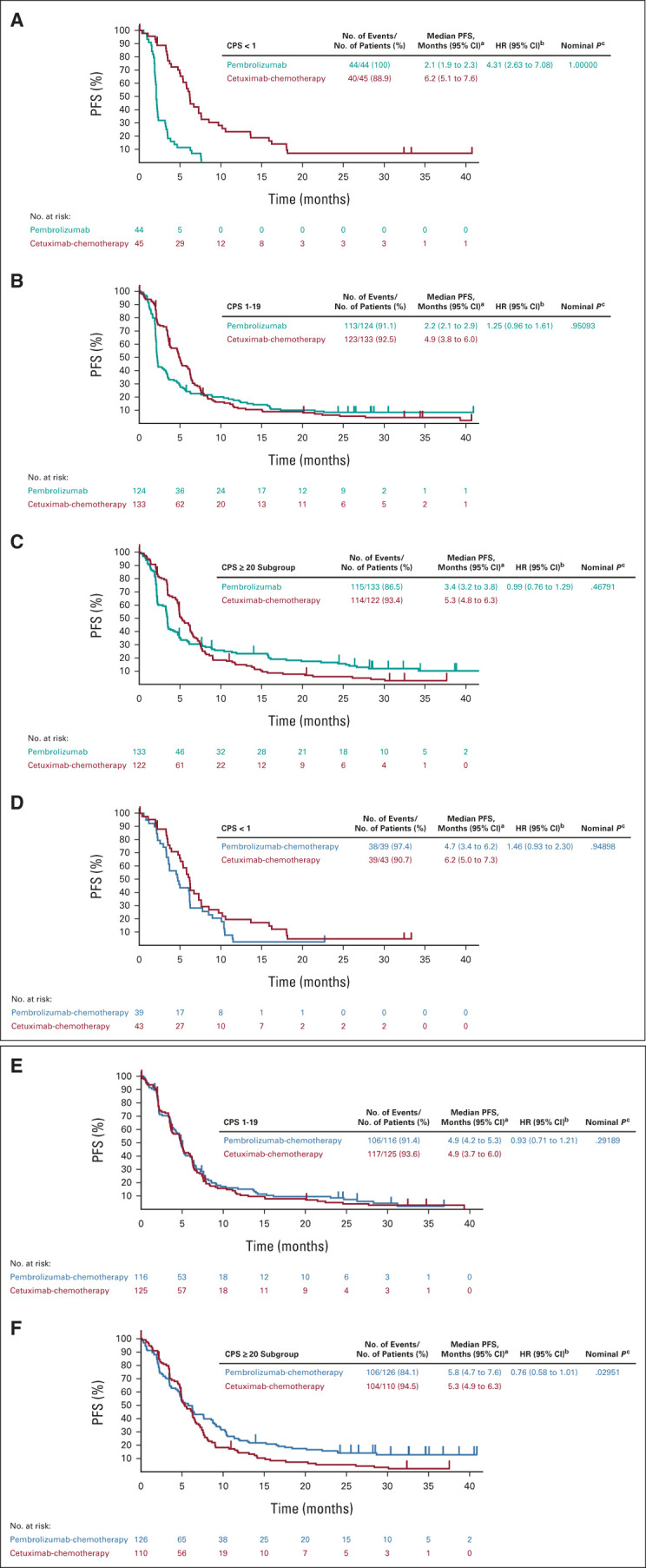
Methods: Participants with R/M HNSCC and no prior systemic therapy for R/M disease were randomly assigned 1:1:1 to pembrolizumab, pembrolizumab-chemotherapy, or cetuximab-chemotherapy. Post hoc efficacy analyses of the PD-L1 CPS < 1 and CPS 1-19 subgroups were performed.
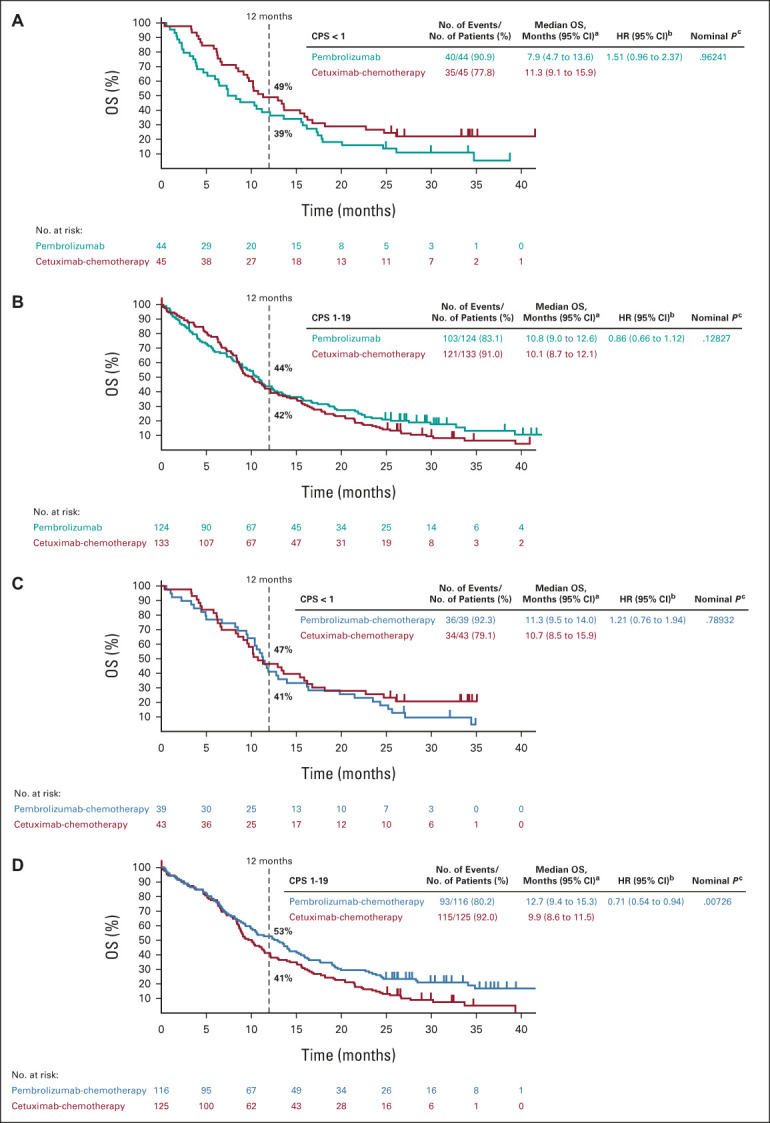
Results: Of 882 participants enrolled, 128 had PD-L1 CPS < 1 and 373 had CPS 1-19. For pembrolizumab versus cetuximab-chemotherapy, the median overall survival was 7.9 versus 11.3 months in the PD-L1 CPS < 1 subgroup (hazard ratio [HR], 1.51 [95% CI, 0.96 to 2.37]) and 10.8 versus 10.1 months in the CPS 1-19 subgroup (HR, 0.86 [95% CI, 0.66 to 1.12]). For pembrolizumab-chemotherapy versus cetuximab-chemotherapy, the median overall survival was 11.3 versus 10.7 months in the PD-L1 CPS < 1 subgroup (HR, 1.21 [95% CI, 0.76 to 1.94]) and 12.7 versus 9.9 months in the CPS 1-19 subgroup (HR, 0.71 [95% CI, 0.54 to 0.94]).
Conclusion: Increased efficacy of pembrolizumab or pembrolizumab-chemotherapy was observed with increasing PD-L1 expression. PD-L1 CPS < 1 subgroup analysis was limited by small participant numbers. Results from the PD-L1 CPS 1-19 subgroup support previous findings of treatment benefit with pembrolizumab monotherapy and pembrolizumab-chemotherapy in patients with PD-L1 CPS ≥ 1 tumors. Although PD-L1 expression is informative, exploration of additional predictive biomarkers is needed for low PD-L1-expressing HNSCC.
Conflict of interest statement
This author is a member of the
No other potential conflicts of interest were reported.
Figures
References
-
- Seiwert TY, Burtness B, Mehra R, et al. : Safety and clinical activity of pembrolizumab for treatment of recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-012): An open-label, multicentre, phase 1b trial. Lancet Oncol 17:956-965, 2016 - PubMed
-
- Patel SP, Kurzrock R: PD-L1 expression as a predictive biomarker in cancer immunotherapy. Mol Cancer Ther 14:847-856, 2015 - PubMed
-
- Sharpe AH, Wherry EJ, Ahmed R, et al. : The function of programmed cell death 1 and its ligands in regulating autoimmunity and infection. Nat Immunol 8:239-245, 2007 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
