

Prehospital traumatic cardiac arrest: a systematic review and meta-analysis
- PMID: 35333932
- PMCID: PMC9360068
- DOI: 10.1007/s00068-022-01941-y
Prehospital traumatic cardiac arrest: a systematic review and meta-analysis
Erratum in
-
Correction to: Prehospital traumatic cardiac arrest: a systematic review and meta-analysis.Eur J Trauma Emerg Surg. 2022 Aug;48(4):3373. doi: 10.1007/s00068-022-01975-2. Eur J Trauma Emerg Surg. 2022. PMID: 35511241 Free PMC article. No abstract available.
Abstract
Background: Circulatory arrest after trauma is a life-threatening situation that mandates urgent action. The aims of this systematic review and meta-analysis on prehospital traumatic cardiac arrest (TCA) were to provide an updated pooled mortality rate for prehospital TCA, to investigate the impact of the time of patient inclusion and the type of prehospital trauma system on TCA mortality rates and neurological outcome, and to investigate which pre- and intra-arrest factors are prognostic for prehospital TCA mortality.
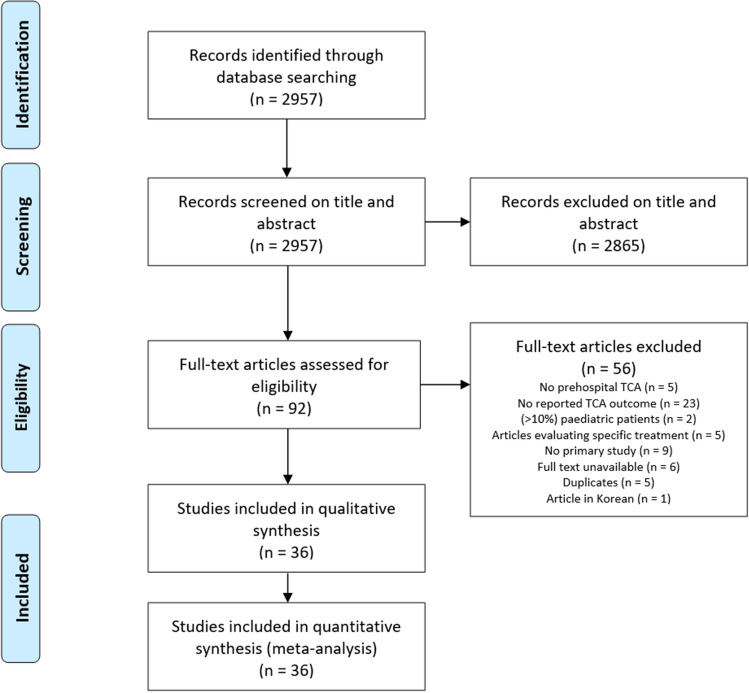
Methods: This review was conducted in accordance with the PRISMA and CHARMS guidelines. Databases were searched for primary studies published about prehospital TCA patients (1995-2020). Studies were divided into various EMS-system categories. Data were analyzed using MedCalc, Review Manager, Microsoft Excel, and Shinyapps Meta Power Calculator software.
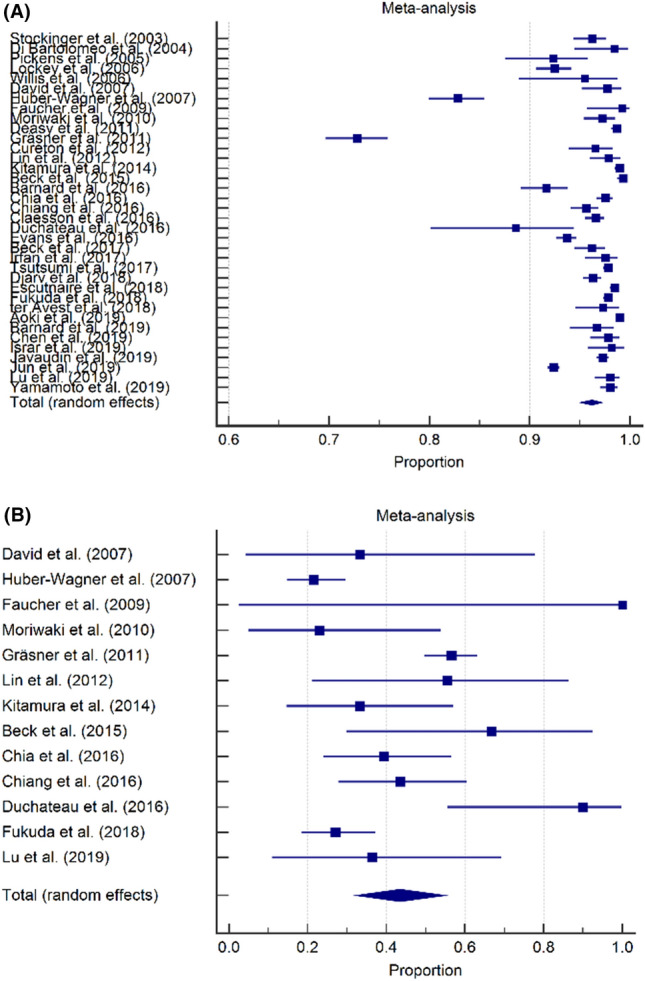
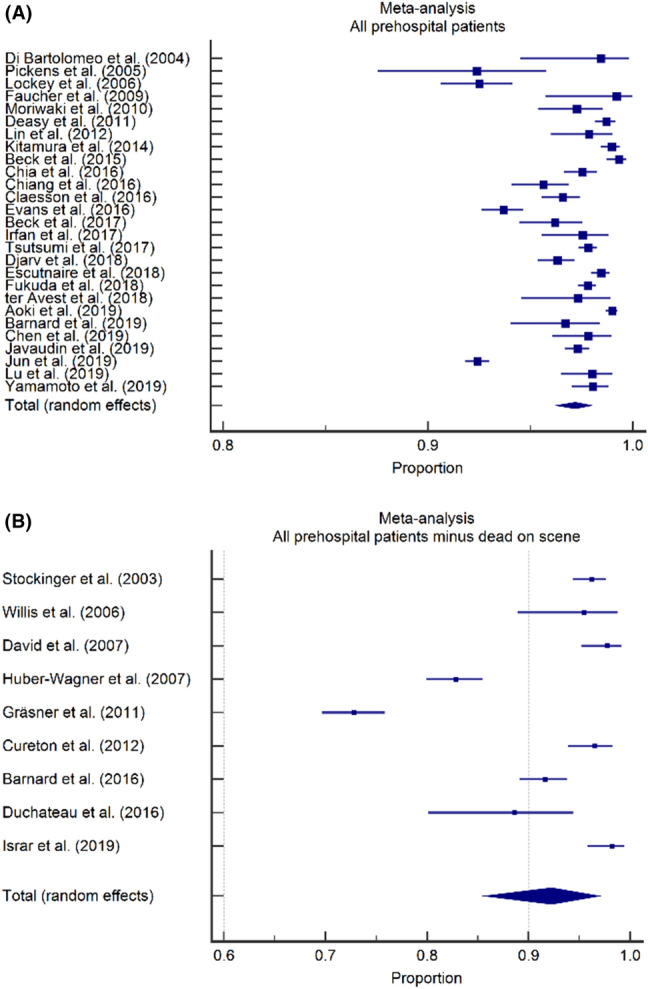
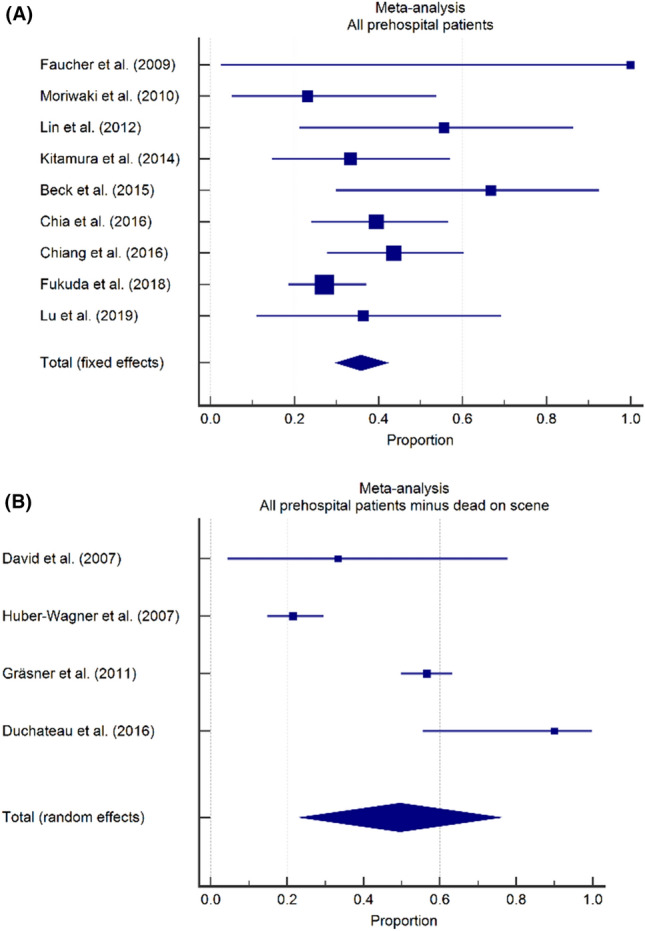
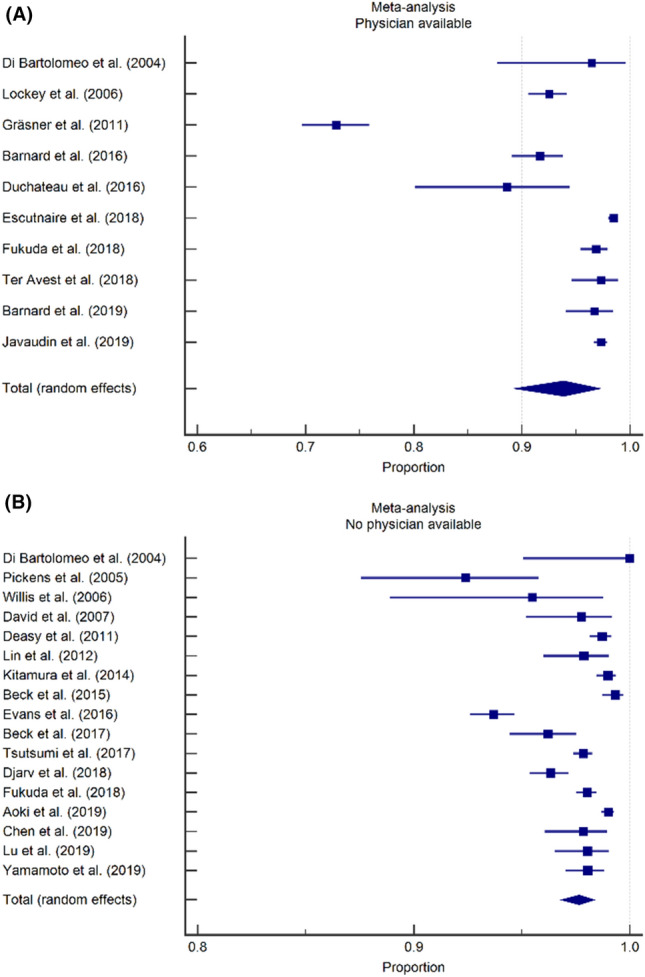
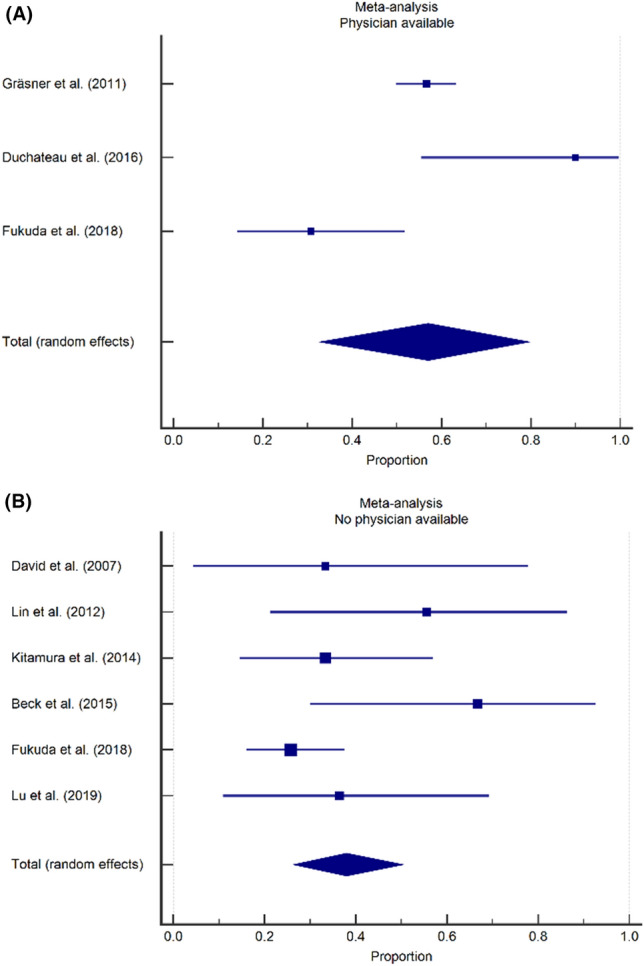
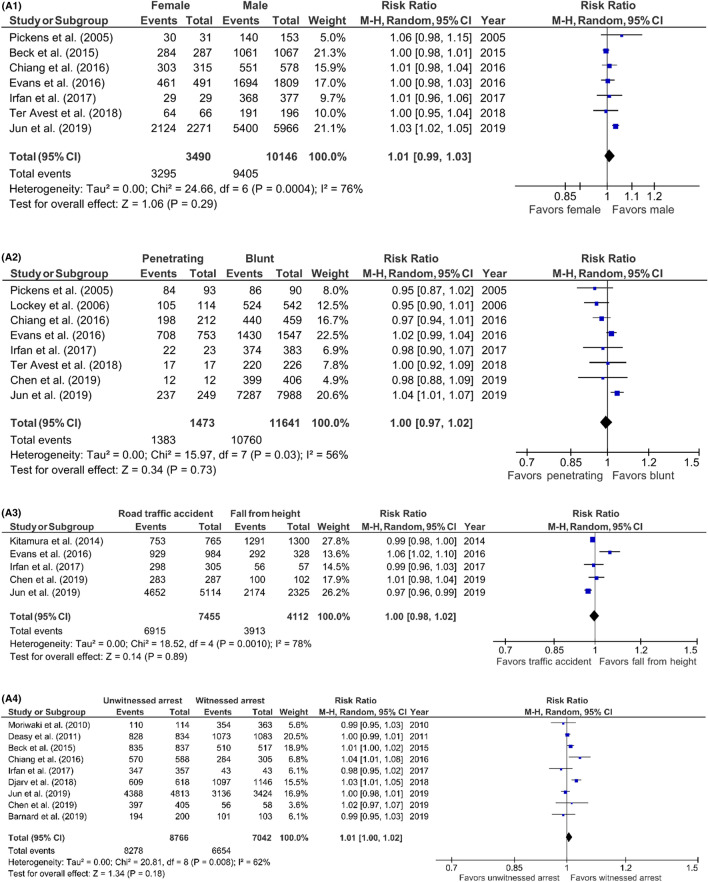
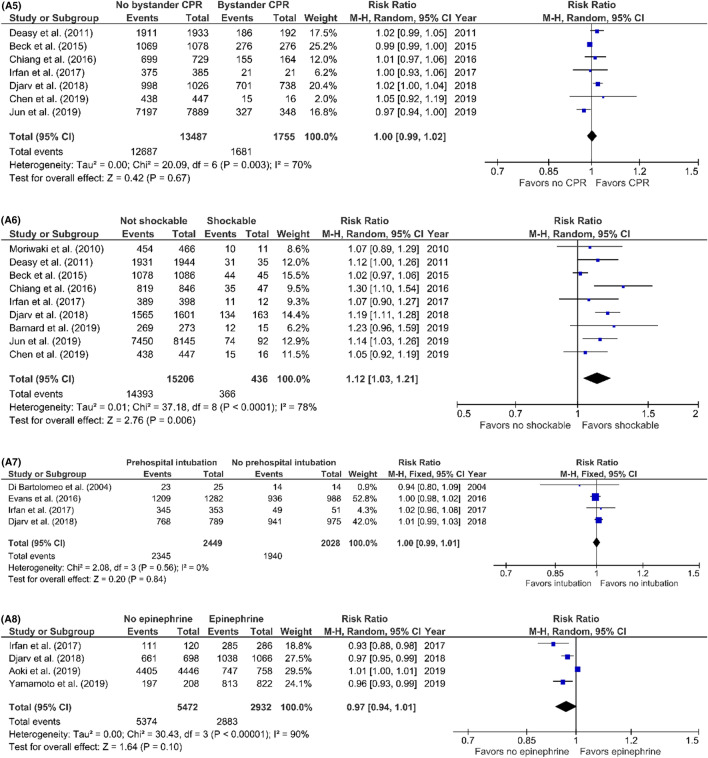
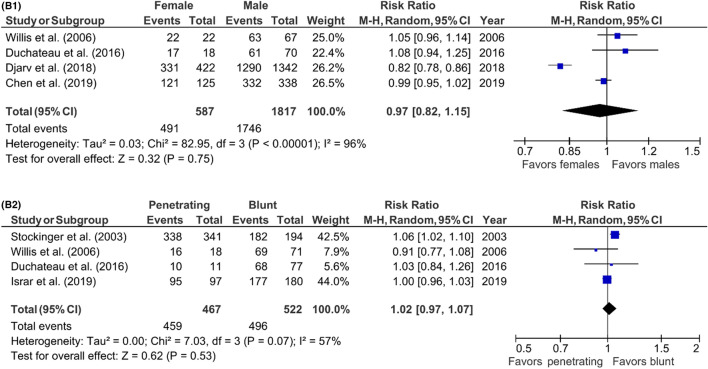
Results: Thirty-six studies involving 51.722 patients were included. Overall mortality for TCA was 96.2% and a favorable neurological outcome was seen in 43.5% of the survivors. Mortality rates were 97.2% in studies including prehospital deaths and 92.3% in studies excluding prehospital deaths. Favorable neurological outcome rates were 35.8% in studies including prehospital deaths and 49.5% in studies excluding prehospital deaths. Mortality rates were 97.6% if no physician was available at the prehospital scene and 93.9% if a physician was available. Favorable neurological outcome rates were 57.0% if a physician was available on scene and 38.0% if no physician was available. Only non-shockable rhythm was associated with a higher mortality (RR 1.12, p = 0.06).
Conclusion: Approximately 1 in 20 patients with prehospital TCA will survive; about 40% of survivors have favorable neurological outcome.
Keywords: Mortality; Neurological outcome; Organization of EMS system; Prognostic factors; Registry type; Traumatic cardiac arrest (TCA).
© 2022. The Author(s).
Conflict of interest statement
There are no conflicts of interest in the materials or subject matter dealt with the manuscript.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
