

Total Endovascular Aortic Arch Repair: From Dream to Reality
- PMID: 35334549
- PMCID: PMC8948628
- DOI: 10.3390/medicina58030372
Total Endovascular Aortic Arch Repair: From Dream to Reality
Abstract
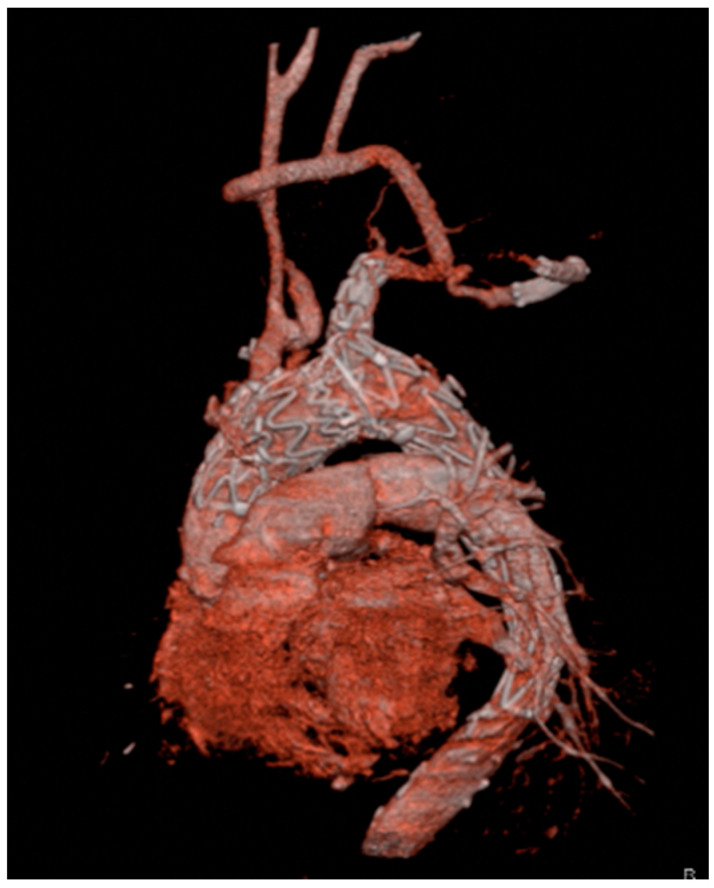
The gold-standard therapy for the treatment of aortic arch pathologies is conventional open surgery. Recently, total endovascular aortic arch replacement with branched stent-grafts has been introduced into clinical practice with the aim of reducing invasiveness especially in selected high-risk patients. The aim of this review is to describe the two most commonly used branched devices for endovascular arch stent-grafting: Nexus (Endospan, Herzlia, Israle) and RelayBranch (Terumo Aortic, Glasgow, United Kingdom). Nexus is a CE-certified off-the-shelf, single branch, double stent graft system. It consists of two different components: a main module for the aortic arch and the descending aorta with a side-branch for the brachiocephalic artery (BCA), and a curved module for the ascending aorta that lands into the sino-tubular junction and connects to the main module through a side-facing self-protecting sleeve. Nexus may be used in urgent-emergency cases and also in patients with only one suitable supra-aortic target vessel but, on the other hand, it makes cerebral blood flow dependent on one source vessel only. The RelayBranch Thoracic Stent-Graft System is a custom made, double branched endograft with a wide window on its superior portion to accommodate two inner tunnels for BCA and left common carotid artery connection; bilateral cervical accesses are generally used to advance guidewires for catheterization of the inner tunnels in a retrograde fashion. RelayBranch can be customized on every patient's specific anatomy and provides a double blood source for the brain, but it cannot be used in urgent-emergency conditions. Therefore, in order to optimize outcomes, the choice of the most appropriate device should be made considering pros and cons of each system and patient's anatomy by an experienced aortic team. In conclusion, total endovascular aortic arch exclusion is a promising reality in selected high-risk patients.
Keywords: aortic arch pathologies; aortic arch stent-grafting; endovascular procedures.
Conflict of interest statement
The authors declare no conflict of interest.
Figures



References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
