

SARS-CoV-2 Omicron Symptomatic Infections in Previously Infected or Vaccinated South African Healthcare Workers
- PMID: 35335091
- PMCID: PMC8951475
- DOI: 10.3390/vaccines10030459
SARS-CoV-2 Omicron Symptomatic Infections in Previously Infected or Vaccinated South African Healthcare Workers
Abstract
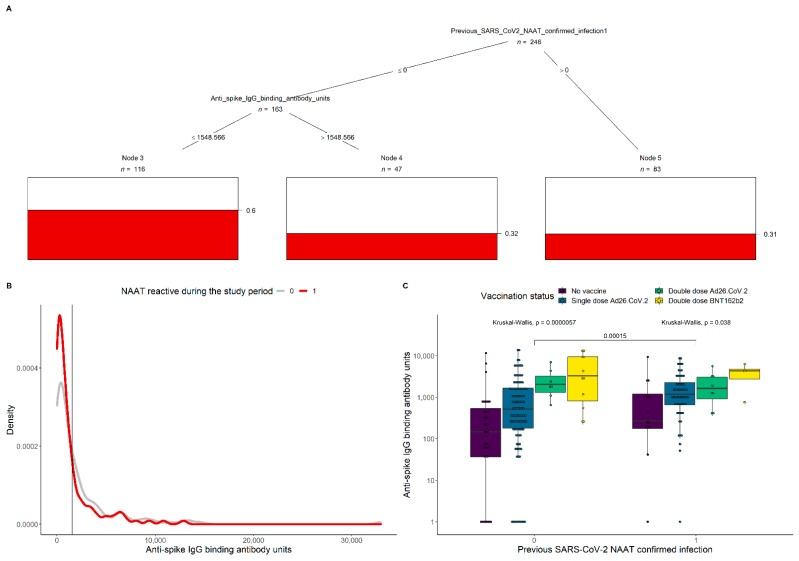
We investigated Omicron infections among healthcare workers (HCW) presenting with symptoms of SARS-CoV-2 infection and evaluated the protective effect of vaccination or prior infection. Between 24 November and 31 December 2021, HCW in Johannesburg, South Africa, were tested for SARS-CoV-2 infection by Nucleic Acid Amplification Test (NAAT). Blood samples collected either at the symptomatic visit or in the 3 months prior, were tested for spike protein immunoglobulin G (IgG). Overall, 433 symptomatic HCW were included in the analysis, with 190 (43.9%) having an Omicron infection; 69 (16.7%) were unvaccinated and 270 (62.4%) received a single dose of the Ad26.COV.2 vaccine. There was no difference in the odds of identifying Omicron between unvaccinated and Ad26.COV.2 vaccinated HCW (adjusted odds ratio (aOR) 0.81, 95% confidence interval (CI): 0.46, 1.43). One-hundred and fifty-four (35.3%) HCW had at least one SARS-CoV-2 NAAT-confirmed prior infection; these had lower odds of Omicron infection compared with those without past infection (aOR 0.55, 95%CI: 0.36, 0.84). Anti-spike IgG concentration of 1549 binding antibody unit/mL was suggestive of significant reduction in the risk of symptomatic Omicron infection. We found high reinfection and vaccine breakthrough infection rates with the Omicron variant among HCW. Prior infection and high anti-spike IgG concentration were protective against Omicron infection.
Keywords: COVID-19; Omicron; SARS-CoV-2; reinfection; vaccination.
Conflict of interest statement
M.C.N. reports grants from the Bill & Melinda Gates Foundation, European & Developing Countries Clinical Trials Partnership, Pfizer, AstraZeneca, and Sanofi-Pasteur; and personal fees from Pfizer and Sanofi-Pasteur. S.A.M. reports grants and personal fees from the Bill & Melinda Gates Foundation, and grants from the South African Medical Research Council, Novavax, Pfizer, Minervax, and European & Developing Countries Clinical Trials Partnership. G.K. reports grants from the Bill & Melinda Gates Foundation.
Figures
References
-
- Tracking SARS-COV-2 Variants. [(accessed on 19 January 2022)]. Available online: https://www.nicd.ac.za/diseases-a-z-index/disease-index-covid-19/sars-co...
-
- Gray G.E., Collie S., Garrett N., Goga A., Champion J., Zylstra M., Reddy T., Yende N., Seocharan I., Takalani A., et al. Vaccine effectiveness against hospital admission in South African health care workers who received a homologous booster of Ad26.COV2 during an Omicron COVID19 wave: Preliminary Results of the Sisonke 2 Study. medRxiv. 2021 doi: 10.1101/2021.12.28.21268436. - DOI
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
