

A Novel Concept of Combined High-Level-Laser Treatment and Transcutaneous Photobiomodulation Therapy Utilisation in Orthodontic Periodontal Interface Management
- PMID: 35336433
- PMCID: PMC8951072
- DOI: 10.3390/s22062263
A Novel Concept of Combined High-Level-Laser Treatment and Transcutaneous Photobiomodulation Therapy Utilisation in Orthodontic Periodontal Interface Management
Abstract
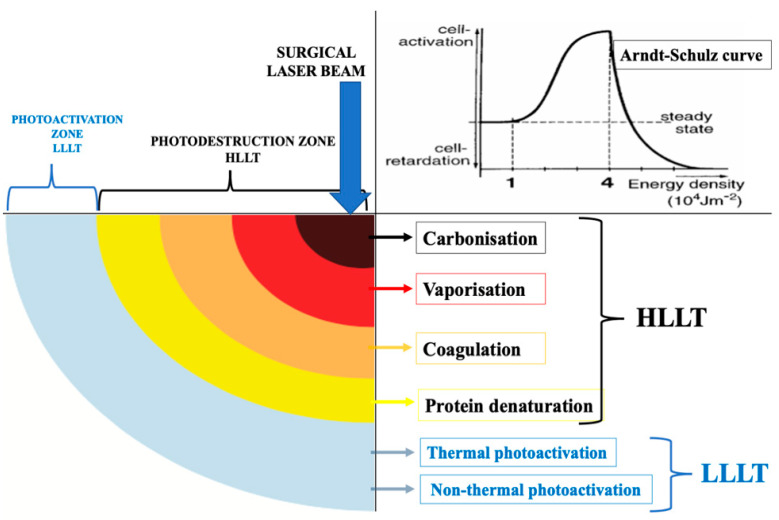
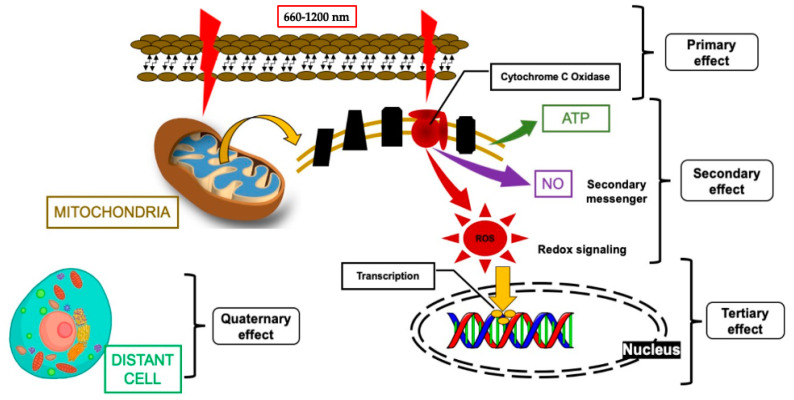
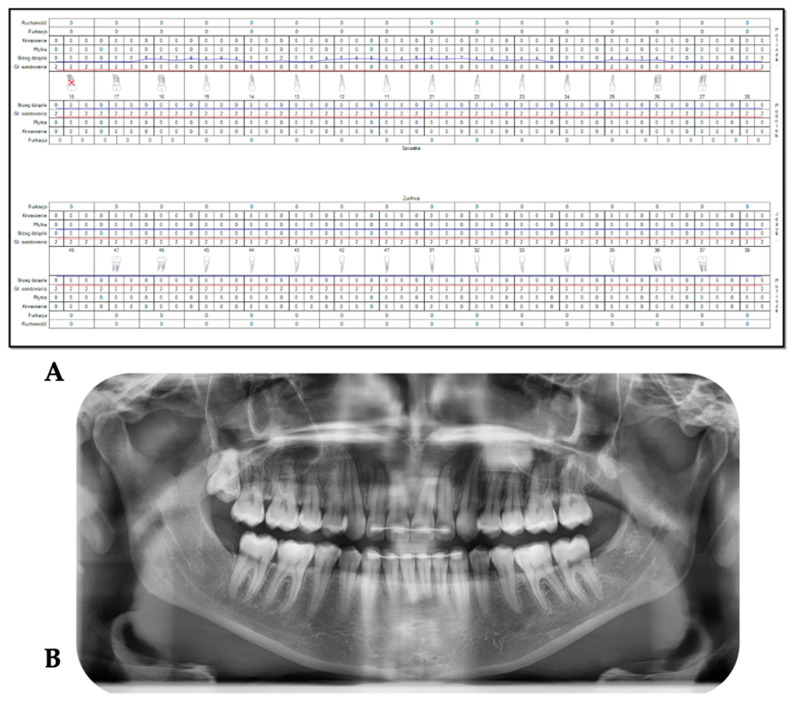
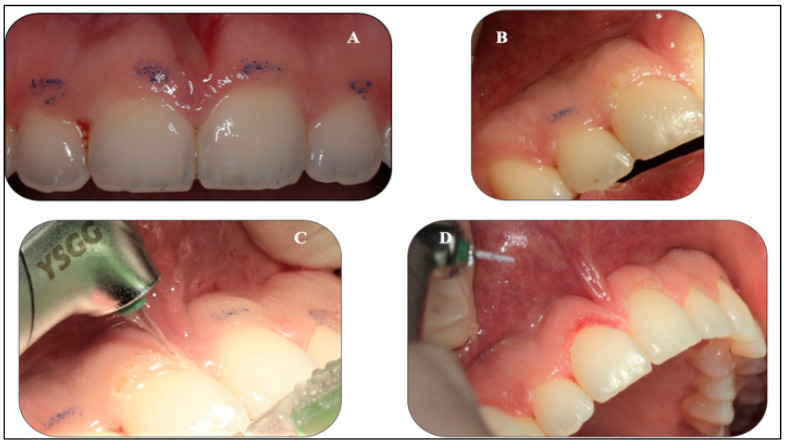
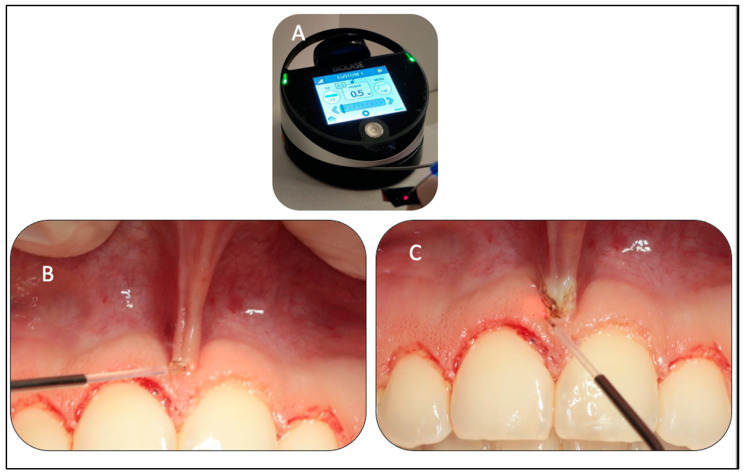
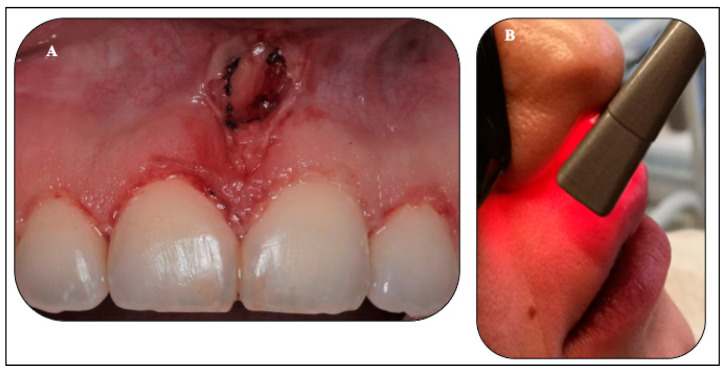
This case report is aimed to demonstrate the synergetic effects of λ940 nm laser photobiomodulation (PBM) therapy in augmenting the advantages of high-level-laser treatment (HLLT)-mediated reaction orthodontic periodontal interface management. Materials and Methods: A 32-year-old female who presented with a persistent gummy smile of upper incisors and low upper midline frenum attachment post-orthodontic treatment, was seeking a better smile appearance. She had a history of delayed wound healing without underlying medical conditions; otherwise, she was fit and healthy. She underwent laser ablation of the upper midline frenum and gingivoplasty of the upper incisors region with λ940 nm and λ2780, respectively, as well as transcutaneous PBM therapy (λ940 nm) to accelerate wound healing. The laser protocols were as follows: λ2780 nm: power output-2 W, pulse width-60 μs, free running pulse (FRP), spot area-0.0016 cm2, pulse repetition rate-25 pulses per second (s), 80 mJ/pulse, 90 s, λ940 nm: 1.2 W, continuous wave (CW) emission mode, 300 μm, 60 s; whereas the adjunctive λ940 nm induced-PBM parameters were as follows: power output-1.4 W, CW-120 s, single application, spot area-2.8 cm2. An acceleration of the wound healing was observed on the 4th day of treatment with no immediate or post-operative complications. The results showed no functional or aesthetic relapses at a long-term follow-up of 6 months. The authors concluded that λ940 nm laser-PBM can provide a synergetic effect to HLLT in accelerating wound healing and offering a precision smile with minimal to none post-operative complications. It is safe and justifiable to utilise dual therapy over the conventional methods, which serves our patients' needs in our daily practice and in various clinical indications. The concept and laser protocols of this clinical case report can pave the roadmap for future extensive studies.
Keywords: Er,Cr:YSGG; HLLT; LLLT; PBM; gingivoplasty; oral wound regeneration; photochemical; photothermal; surgical diode laser; upper midline frenectomy.
Conflict of interest statement
All authors have declared no conflict of interest.
Figures





References
-
- Bhatsange A., Meshram E.P., Waghamare A., Shiggaon L., Mehetre V.N., Shende A. A clinical and histological comparison of mucosal incisions produced by scalpel, electrocautery, and diode laser: A pilot study. J. Dent. Lasers. 2016;10:37–42. doi: 10.4103/2321-1385.196962. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
