

Application of Wearable Sensors Technology for Lumbar Spine Kinematic Measurements during Daily Activities following Microdiscectomy Due to Severe Sciatica
- PMID: 35336772
- PMCID: PMC8945562
- DOI: 10.3390/biology11030398
Application of Wearable Sensors Technology for Lumbar Spine Kinematic Measurements during Daily Activities following Microdiscectomy Due to Severe Sciatica
Abstract
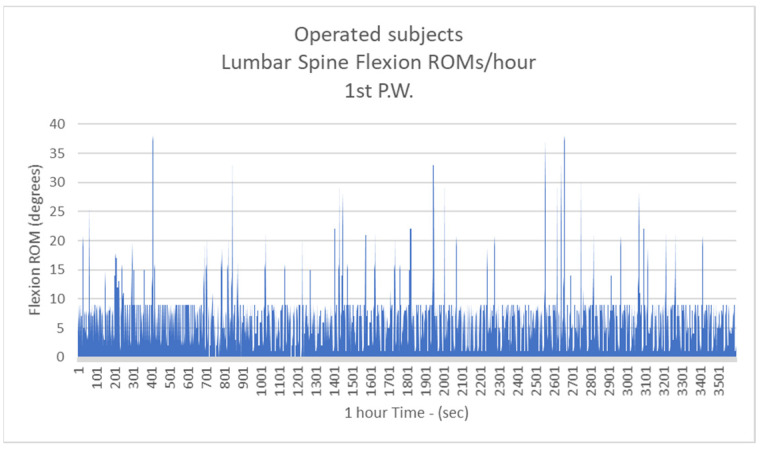
Background: The recurrence rate of lumbar spine microdiscectomies (rLSMs) is estimated to be 5-15%. Lumbar spine flexion (LSF) of more than 10° is mentioned as the most harmful load to the intervertebral disc that could lead to recurrence during the first six postoperative weeks. The purpose of this study is to quantify LSFs, following LSM, at the period of six weeks postoperatively.
Methods: LSFs were recorded during the daily activities of 69 subjects for 24 h twice per week, using Inertial Measurement Units (IMU).
Results: The mean number of more than 10 degrees of LSFs per hour were: 41.3/h during the 1st postoperative week (P.W.) (29.9% healthy subjects-H.S.), 2nd P.W. 60.1/h (43.5% H.S.), 3rd P.W. 74.2/h (53.7% H.S.), 4th P.W. 82.9/h (60% H.S.), 5th P.W. 97.3/h (70.4% H.S.) and 6th P.W. 105.5/h (76.4% H.S.).
Conclusions: LSFs constitute important risk factors for rLDH. Our study records the lumbar spine kinematic pattern of such patients for the first time during their daily activities. Patients' data report less sagittal plane movements than healthy subjects. In vitro studies should be carried out, replicating our results to identify if such a kinematic pattern could cause rLDH. Furthermore, IMU biofeedback capabilities could protect patients from such harmful movements.
Keywords: IMU technology; lumbar microdiscectomy; lumbar spine biomechanics; spine biomechanics; wearable sensors.
Conflict of interest statement
The authors declare no conflict of interest.
Figures











References
LinkOut - more resources
Full Text Sources
