

Which features of patients are morally relevant in ventilator triage? A survey of the UK public
- PMID: 35337310
- PMCID: PMC8956145
- DOI: 10.1186/s12910-022-00773-0
Which features of patients are morally relevant in ventilator triage? A survey of the UK public
Abstract
Background: In the early stages of the COVID-19 pandemic, many health systems, including those in the UK, developed triage guidelines to manage severe shortages of ventilators. At present, there is an insufficient understanding of how the public views these guidelines, and little evidence on which features of a patient the public believe should and should not be considered in ventilator triage.
Methods: Two surveys were conducted with representative UK samples. In the first survey, 525 participants were asked in an open-ended format to provide features they thought should and should not be considered in allocating ventilators for COVID-19 patients when not enough ventilators are available. In the second survey, 505 participants were presented with 30 features identified from the first study, and were asked if these features should count in favour of a patient with the feature getting a ventilator, count against the patient, or neither. Statistical tests were conducted to determine if a feature was generally considered by participants as morally relevant and whether its mean was non-neutral.
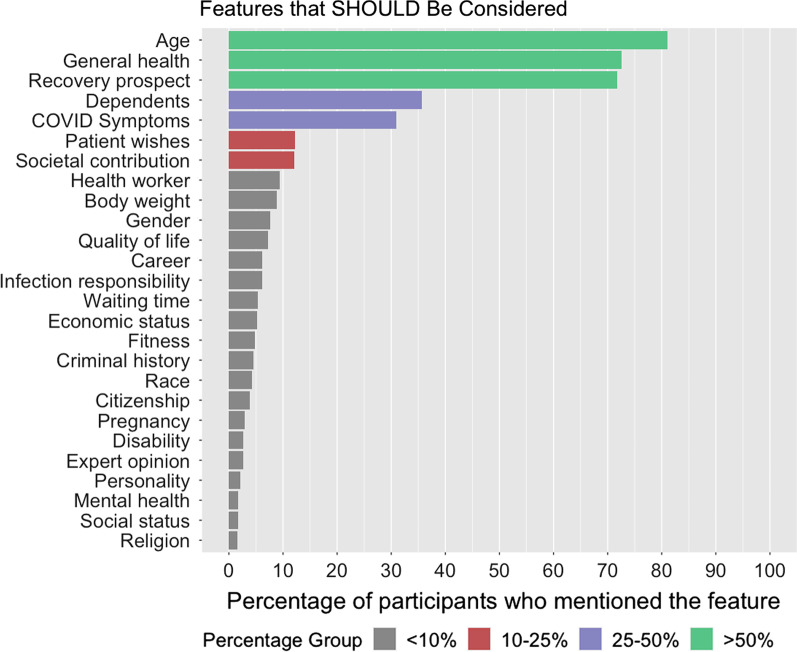
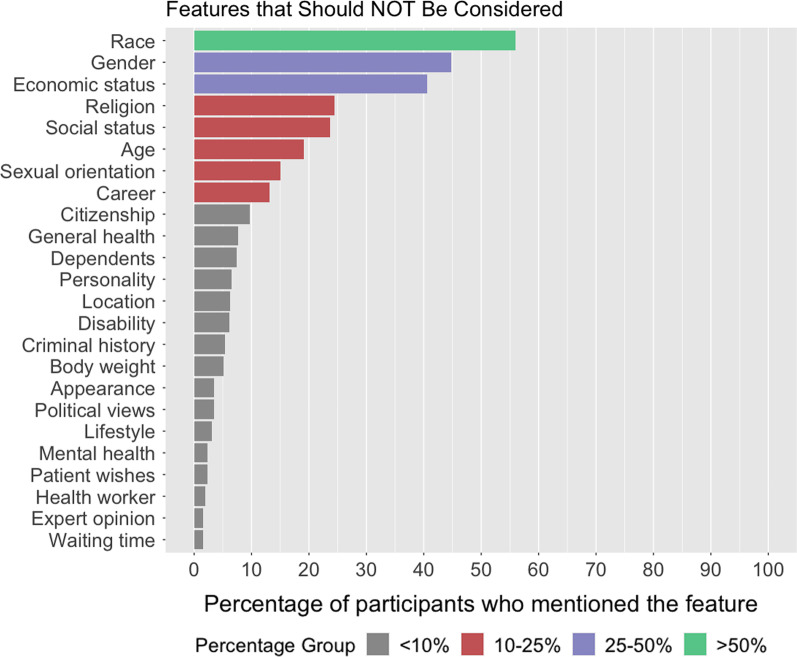
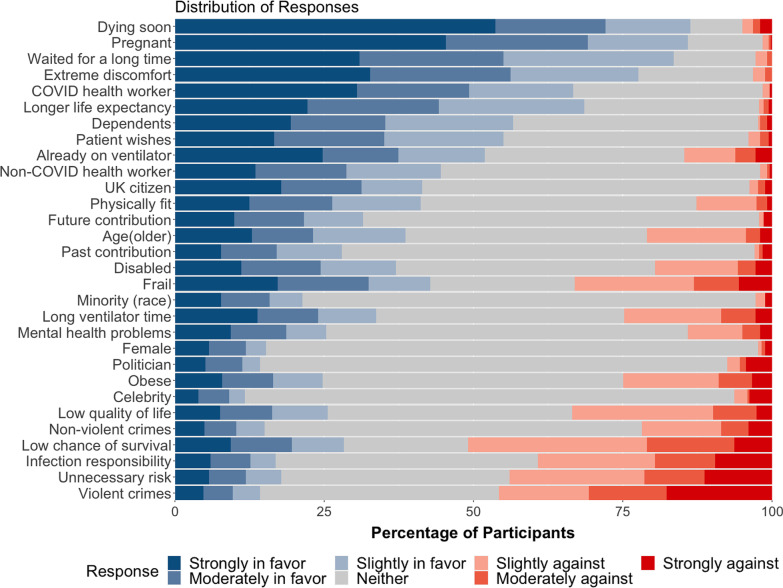
Results: In Survey 1, the features of a patient most frequently cited as being morally relevant to determining who would receive access to ventilators were age, general health, prospect of recovery, having dependents, and the severity of COVID symptoms. The features most frequently cited as being morally irrelevant to determining who would receive access to ventilators are race, gender, economic status, religion, social status, age, sexual orientation, and career. In Survey 2, the top three features that participants thought should count in favour of receiving a ventilator were pregnancy, having a chance of dying soon, and having waited for a long time. The top three features that participants thought should count against a patient receiving a ventilator were having committed violent crimes in the past, having unnecessarily engaged in activities with a high risk of COVID-19 infection, and a low chance of survival.
Conclusions: The public generally agreed with existing UK guidelines that allocate ventilators according to medical benefits and that aim to avoid discrimination based on demographic features such as race and gender. However, many participants expressed potentially non-utilitarian concerns, such as inclining to deprioritise ventilator allocation to those who had a criminal history or who contracted the virus by needlessly engaging in high-risk activities.
Keywords: COVID-19; Medical ethics; Rationing; Scarce resources; Triage.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Allocation of Mechanical Ventilators During a Pandemic: A Mixed-Methods Study of Perceptions Among Japanese Health Care Workers and the General Public.Chest. 2021 Jun;159(6):2494-2502. doi: 10.1016/j.chest.2021.01.015. Epub 2021 Jan 11. Chest. 2021. PMID: 33444616
-
Race and resource allocation: an online survey of US and UK adults' attitudes toward COVID-19 ventilator and vaccine distribution.BMJ Open. 2022 Nov 21;12(11):e062561. doi: 10.1136/bmjopen-2022-062561. BMJ Open. 2022. PMID: 36410823 Free PMC article.
-
Public Opinion on Priorities Toward Fair Allocation of Ventilators During COVID-19 Pandemic: A Nationwide Survey.Front Public Health. 2021 Dec 14;9:753048. doi: 10.3389/fpubh.2021.753048. eCollection 2021. Front Public Health. 2021. PMID: 34970524 Free PMC article.
-
A catalogue of tools and variables from crisis and routine care to support decision-making about allocation of intensive care beds and ventilator treatment during pandemics: Scoping review.J Crit Care. 2021 Dec;66:33-43. doi: 10.1016/j.jcrc.2021.08.001. Epub 2021 Aug 23. J Crit Care. 2021. PMID: 34438132
-
Variation in Ventilator Allocation Guidelines by US State During the Coronavirus Disease 2019 Pandemic: A Systematic Review.JAMA Netw Open. 2020 Jun 1;3(6):e2012606. doi: 10.1001/jamanetworkopen.2020.12606. JAMA Netw Open. 2020. PMID: 32558916 Free PMC article.
Cited by
-
Explicit discrimination and ingroup favoritism, but no implicit biases in hypothetical triage decisions during COVID-19.Sci Rep. 2024 Jan 12;14(1):1213. doi: 10.1038/s41598-023-50385-w. Sci Rep. 2024. PMID: 38216652 Free PMC article.
-
Collective Reflective Equilibrium, Algorithmic Bioethics and Complex Ethics.Camb Q Healthc Ethics. 2025 Apr;34(2):204-219. doi: 10.1017/S0963180124000719. Camb Q Healthc Ethics. 2025. PMID: 39895279 Free PMC article.
-
Justification of principles for healthcare priority setting: the relevance and roles of empirical studies exploring public values.J Med Ethics. 2025 Mar 26;51(4):285-292. doi: 10.1136/jme-2022-108702. J Med Ethics. 2025. PMID: 36813548 Free PMC article.
-
What are the views of Quebec and Ontario citizens on the tiebreaker criteria for prioritizing access to adult critical care in the extreme context of a COVID-19 pandemic?BMC Med Ethics. 2024 Mar 19;25(1):31. doi: 10.1186/s12910-024-01030-2. BMC Med Ethics. 2024. PMID: 38504267 Free PMC article.
-
Public voices on tie-breaking criteria and underlying values in COVID-19 triage protocols to access critical care: a scoping review.Discov Health Syst. 2023;2(1):16. doi: 10.1007/s44250-023-00027-9. Epub 2023 May 10. Discov Health Syst. 2023. PMID: 37206881 Free PMC article.
References
-
- Maves RC, Downar J, Dichter JR, Hick JL, Devereaux A, Geiling JA, Kissoon N, Hupert N, Niven AS, King MA, Rubinson LL, Hanfling D, Hodge JG, Jr, Marshall MF, Fischkoff K, Evans LE, Tonelli MR, Wax RS, Seda G, Parrish JS, Truog RD, Sprung CL, Christian MD. ACCP task force for mass critical care. Triage of scarce critical care resources in COVID-19 an implementation guide for regional allocation: an expert panel report of the task force for mass critical care and the American College of Chest Physicians. Chest. 2020;158(1):212–225. doi: 10.1016/j.chest.2020.03.063. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
