

Cough-Specific Quality of Life Predicts Disease Progression Among Patients With Interstitial Lung Disease: Data From the Pulmonary Fibrosis Foundation Patient Registry
- PMID: 35337809
- PMCID: PMC9808640
- DOI: 10.1016/j.chest.2022.03.025
Cough-Specific Quality of Life Predicts Disease Progression Among Patients With Interstitial Lung Disease: Data From the Pulmonary Fibrosis Foundation Patient Registry
Abstract
Background: Cough is a common symptom of interstitial lung disease (ILD) and negatively impacts health-related quality of life (QOL). Previous studies have shown that among patients with idiopathic pulmonary fibrosis, cough may predict progression of lung disease and perhaps even respiratory hospitalizations and mortality.
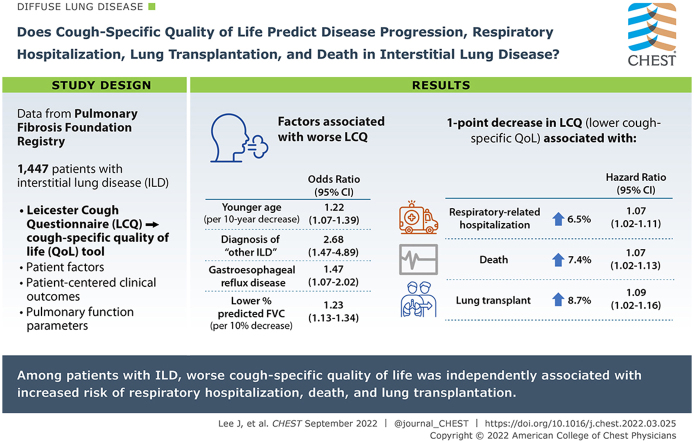
Research question: Does cough-specific QOL predict disease progression, respiratory hospitalization, lung transplantation, and death among patients with ILD?
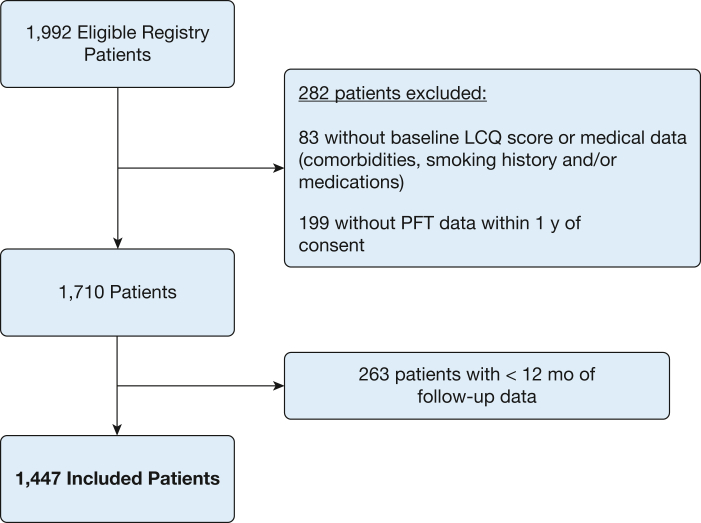
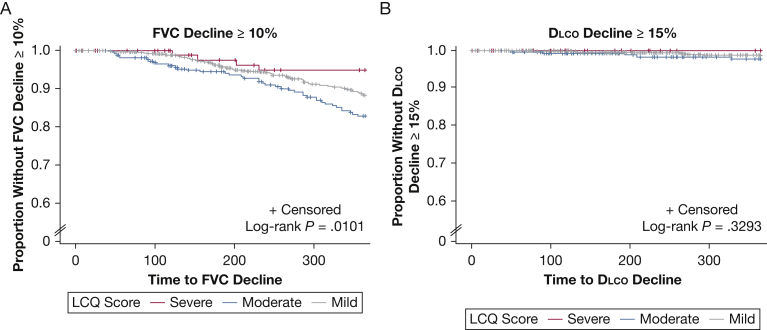
Study design and methods: We analyzed data from the Pulmonary Fibrosis Foundation Registry, which comprises a multicenter population of well-characterized patients with ILD. We first examined associations between patient factors and baseline scores on the Leicester Cough Questionnaire (LCQ), a cough-specific QOL tool, using a proportional odds model. Next, we examined associations between baseline LCQ scores and patient-centered clinical outcomes, as well as pulmonary function parameters, using a univariable and multivariable proportional hazards model that was adjusted for clinically relevant variables, including measures of disease severity.
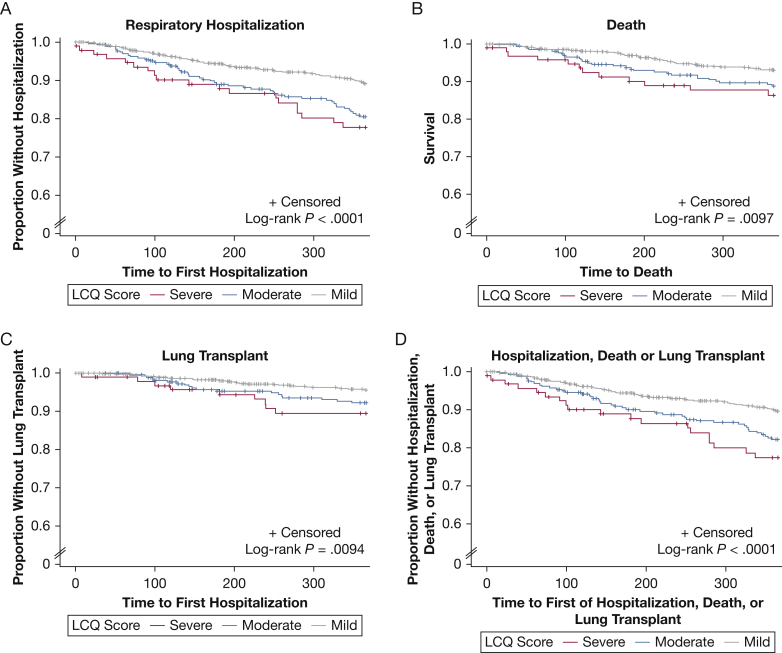
Results: One thousand four hundred forty-seven patients with ILD were included in our study. In the multivariable proportional odds model, we found that the following patient factors were associated with worse cough-specific QOL: younger age, diagnosis of "other ILD," gastroesophageal reflux disease, and lower FVC % predicted. Multivariable Cox regression models, adjusting for several variables including baseline disease severity, showed that a 1-point decrease in LCQ score (indicating lower cough-specific QOL) was associated with a 6.5% higher risk of respiratory-related hospitalization (hazard ratio [HR], 1.065; 95% CI, 1.025-1.107), a 7.4% higher risk of death (HR, 1.074; 95% CI, 1.020-1.130), and an 8.7% higher risk of lung transplantation (HR, 1.087; 95% CI, 1.022-1.156).
Interpretation: Among a large population of well-characterized patients with ILD, cough-specific QOL was associated independently with respiratory hospitalization, death, and lung transplantation.
Keywords: Leicester cough questionnaire; cough; disease progression; health-related quality of life; idiopathic pulmonary fibrosis; interstitial lung disease; mortality.
Copyright © 2022 American College of Chest Physicians. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
The Curious Case of Cough in Interstitial Lung Diseases.Chest. 2022 Sep;162(3):501-502. doi: 10.1016/j.chest.2022.04.139. Chest. 2022. PMID: 36088087 No abstract available.
References
-
- Sumner H., Woodcock A., Kolsum U., et al. Predictors of objective cough frequency in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2013;187(9):943–949. - PubMed
-
- Yount S.E., Beaumont J.L., Chen S.Y., et al. Health-related quality of life in patients with idiopathic pulmonary fibrosis. Lung. 2016;194(2):227–234. - PubMed
