

Acute Kidney Injury in Critically Ill Patients with Cancer
- PMID: 35338071
- PMCID: PMC9625110
- DOI: 10.2215/CJN.15681221
Acute Kidney Injury in Critically Ill Patients with Cancer
Abstract
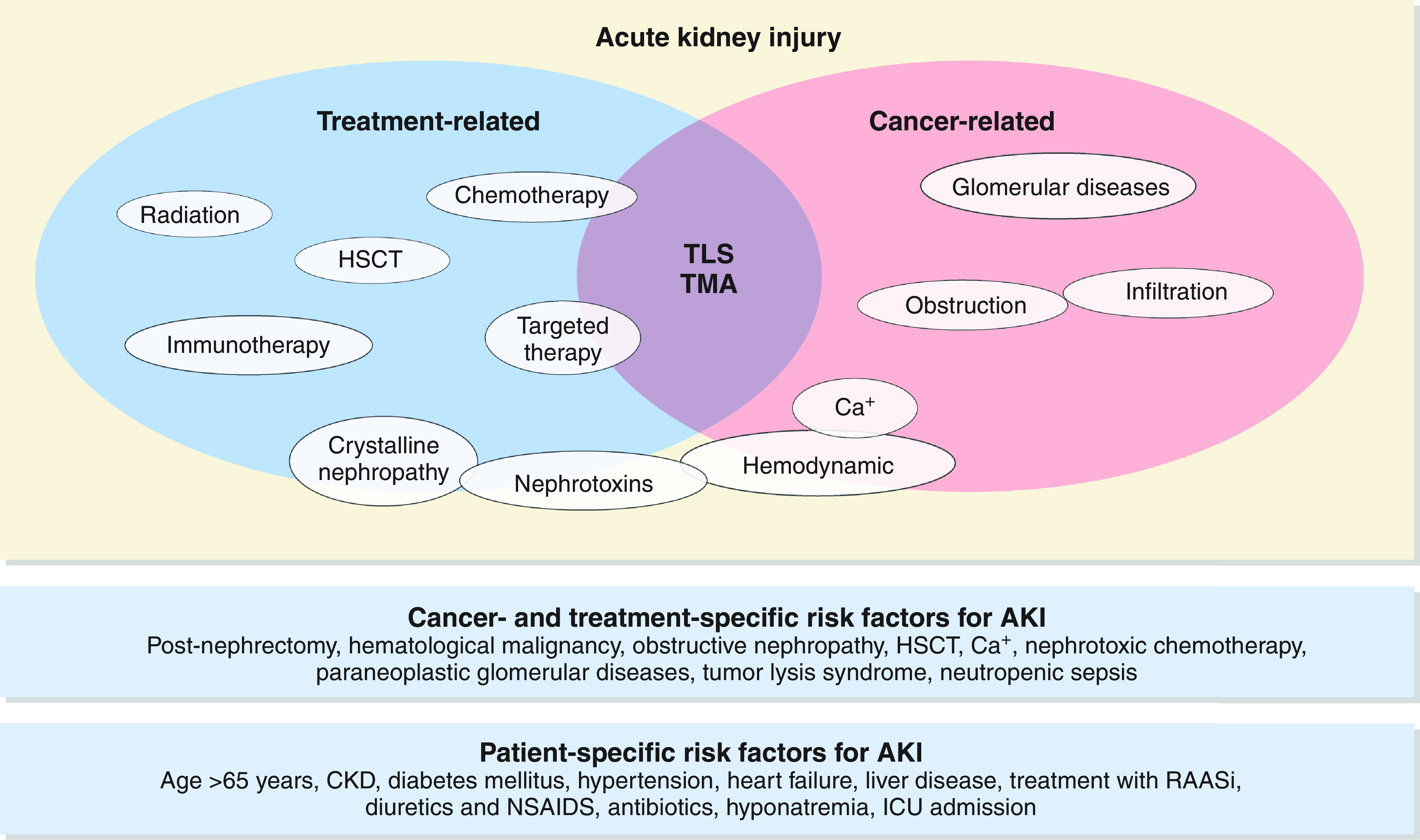
Advances in cancer therapy have significantly improved overall patient survival; however, AKI remains a common complication in patients with cancer, occurring in anywhere from 11% to 22% of patients, depending on patient-related or cancer-specific factors. Critically ill patients with cancer as well as patients with certain malignancies (e.g., leukemias, lymphomas, multiple myeloma, and renal cell carcinoma) are at highest risk of developing AKI. AKI may be a consequence of the underlying malignancy itself or from the wide array of therapies used to treat it. Cancer-associated AKI can affect virtually every compartment of the nephron and can present as subclinical AKI or as overt acute tubular injury, tubulointerstitial nephritis, or thrombotic microangiopathy, among others. AKI can have major repercussions for patients with cancer, potentially jeopardizing further eligibility for therapy and leading to greater morbidity and mortality. This review highlights the epidemiology of AKI in critically ill patients with cancer, risk factors for AKI, and common pathologies associated with certain cancer therapies, as well as the management of AKI in different clinical scenarios. It highlights gaps in our knowledge of AKI in patients with cancer, including the lack of validated biomarkers, as well as evidence-based therapies to prevent AKI and its deleterious consequences.
Keywords: AKI; acute kidney injury; cancer; critical care nephrology and acute kidney injury series; drug nephrotoxicity; onconephrology.
Copyright © 2022 by the American Society of Nephrology.
Figures
References
-
- Christiansen CF, Johansen MB, Langeberg WJ, Fryzek JP, Sørensen HT: Incidence of acute kidney injury in cancer patients: A Danish population-based cohort study. Eur J Intern Med 22: 399–406, 2011 - PubMed
-
- Soares M, Salluh JI, Carvalho MS, Darmon M, Rocco JR, Spector N: Prognosis of critically ill patients with cancer and acute renal dysfunction. J Clin Oncol 24: 4003–4010, 2006 - PubMed
-
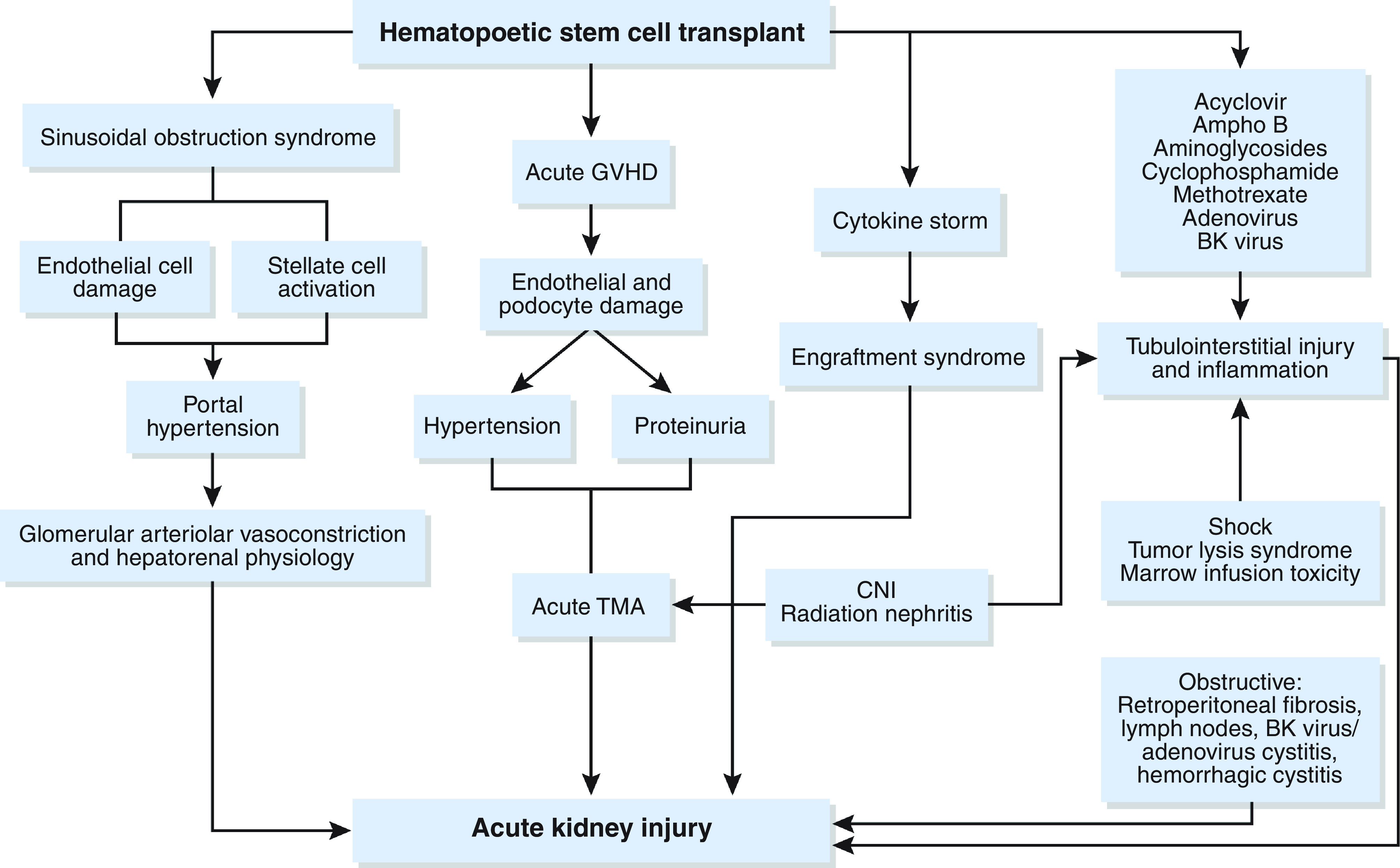
- Parikh CR, McSweeney PA, Korular D, Ecder T, Merouani A, Taylor J, Slat-Vasquez V, Shpall EJ, Jones RB, Bearman SI, Schrier RW: Renal dysfunction in allogeneic hematopoietic cell transplantation. Kidney Int 62: 566–573, 2002 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
