

Reinfection with SARS-CoV-2 in solid-organ transplant recipients: Incidence density and convalescent immunity prior to reinfection
- PMID: 35338554
- PMCID: PMC9115288
- DOI: 10.1111/tid.13827
Reinfection with SARS-CoV-2 in solid-organ transplant recipients: Incidence density and convalescent immunity prior to reinfection
Abstract
Background: Long-term protective immunity to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) remains poorly characterized, particularly in solid organ transplant (SOT) patients.
Method: We determined the incidence density of SARS-CoV-2 reinfection in a cohort of adult SOT recipients initially infected between March 1st, 2020 and March 30th, 2021 and included those with initial infection before or after transplantation. Incidence density was the total cases divided by total days after initial diagnosis with active graft.
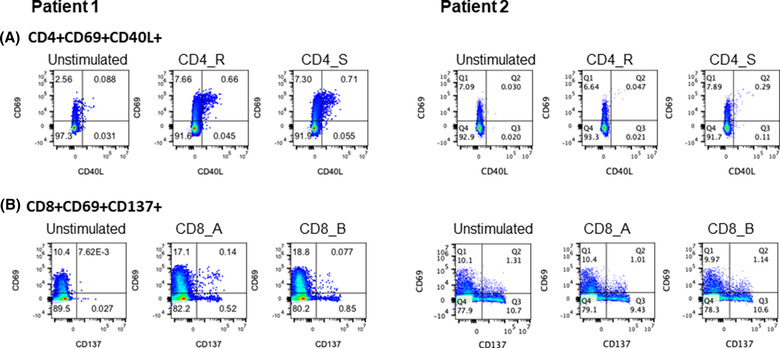
Results: Of 210 infected recipients, five (2.4%) developed reinfection, including two who had received full mRNA vaccination, but none developed hypoxia. The incidence density for reinfection was 9.4 (95% confidence interval [CI] 3.9-22.6) and for primary infection the density was 9.1 (95% CI 7.9-10.5) cases/100,000 patient days. Two recipients had immunity evaluated in the weeks prior to reinfection, by measuring immunoglobulin-G (IgG) antibody titer to the SARS-CoV-2 receptor binding domain and virus-specific CD4+ and CD8+ T-cell reactivity following stimulation with SARS-CoV-2 peptide pools. Both mounted virus specific CD4 T-cell responses prior to reinfection (1.19% and 0.28% of total CD4 T cells) and both had reactive IgG testing (1.30 and 4.99 signal/cut off ratio).
Conclusions: This suggests that SOT recipients infected with SARS-CoV-2 remain at high risk for reinfection even after generating cellular and humoral immune responses.
Keywords: COVID-19; SARS-CoV-2; reinfection; solid organ transplant.
© 2022 Wiley Periodicals LLC.
Conflict of interest statement
The authors of this manuscript have no conflicts of interest to disclose as described by the
Figures
Comment in
-
Comment on "Re-infection with SARS-CoV-2 in solid-organ transplant recipients".Transpl Infect Dis. 2022 Jun;24(3):e13838. doi: 10.1111/tid.13838. Epub 2022 Apr 25. Transpl Infect Dis. 2022. PMID: 35417614 Free PMC article. No abstract available.
-
Response to Letters regarding "Re-infection with SARS-CoV-2 in solid-organ transplant (SOT) recipients: Incidence density and convalescent immunity prior to re-infection".Transpl Infect Dis. 2022 Aug;24(4):e13870. doi: 10.1111/tid.13870. Epub 2022 Jun 1. Transpl Infect Dis. 2022. PMID: 35604781 Free PMC article. No abstract available.
References
-
- Khoury DS, Cromer D, Reynaldi A, et al. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS‐CoV‐2 infection. Nat Med. 2021;27(7):1205‐1211. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
