

Prevalence, management, and outcomes of haemorrhagic events in left ventricular assist device recipients
- PMID: 35338605
- PMCID: PMC9065835
- DOI: 10.1002/ehf2.13899
Prevalence, management, and outcomes of haemorrhagic events in left ventricular assist device recipients
Abstract
Aims: Left ventricular assist devices (LVADs) have reduced the mortality of patients with advanced heart failure both as bridge-to-transplant and as destination therapy. However, LVADs are associated with various complications, including bleedings, which affect the prognosis. The aim of the study was to explore the prevalence, management, and outcomes of haemorrhagic adverse events in LVAD recipients.
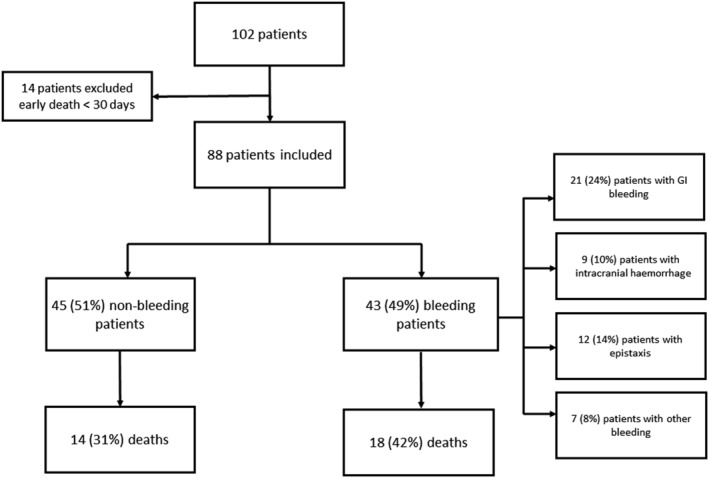
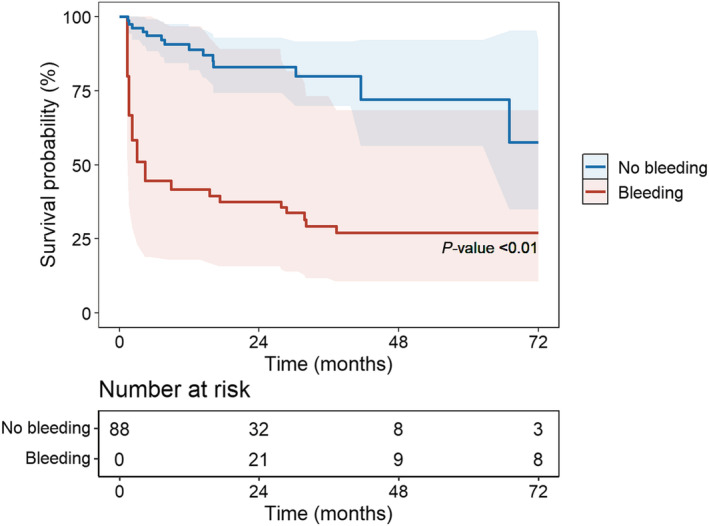
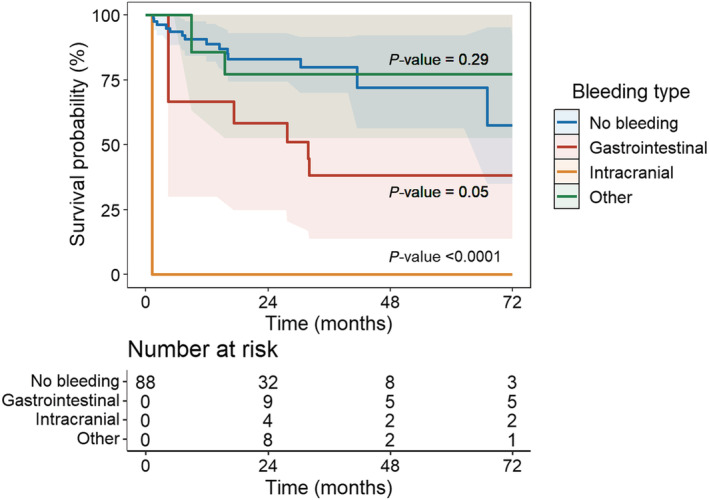
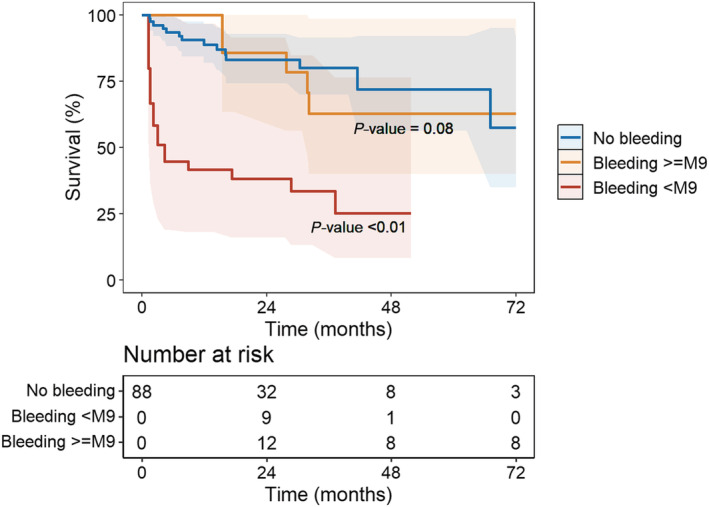
Methods and results: We conducted a retrospective, single-centre, cohort study including all patients who received an LVAD from January 2008 to December 2019 in our tertiary centre (Rangueil University Hospital, Toulouse, France). Bleeding events, death, and heart transplantation were collected from electronic medical files. Eighty-eight patients were included, and 43 (49%) presented at least one bleeding event. Gastrointestinal (GI) bleeding was the most frequent (n = 21, 24%), followed by epistaxis (n = 12, 14%) and intracranial haemorrhage (n = 9, 10%). Bleeding events were associated with increased mortality [hazard ratio (HR) 3.8, 95% confidence interval (CI) 1.5-9.3, P < 0.01], particularly in case of intracranial haemorrhage (HR 14.6, 95% CI 4.2-51.1, P < 0.0001). GI bleedings were associated with a trend towards increased mortality (HR 3.0, 95% CI 0.9-9.3, P = 0.05). Each bleeding episode multiplied the risk of death by 1.8 (95% CI 1.2-2.7, P < 0.01). Finally, only early bleedings (<9 months post-implantation) had an impact on mortality (HR 4.2, 95% CI 1.6-11.1, P < 0.01). Therapeutic management was mainly based on temporary interruption of anticoagulation and permanent interruption of antiplatelet therapy. Invasive management was rarely performed.
Conclusions: Haemorrhagic events in LVAD recipients are frequent and associated with increased mortality. GI bleedings are the most frequent, and intracranial haemorrhages the most associated with mortality. Management remains empirical requiring more research.
Keywords: Bleeding; Heart failure; Left ventricular assist device; Mortality.
© 2022 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
None declared.
Figures
References
-
- DeBakey ME. Left ventricular bypass pump for cardiac assistance. Am J Cardiol. 1971; 27: 3–11. - PubMed
-
- Goldstein DJ, Rose EA. Implantable left ventricular assist devices. N Engl J Med. 1998; 12: 1522–1533. - PubMed
-
- Rose EA, Stevenson LW, Tierney AR. Long‐term use of a left ventricular assist device for end‐stage heart failure. N Engl J Med. 2001; 9: 1435–1443. - PubMed
-
- Miller LW, Pagani FD, Russell SD, John R, Boyle AJ, Aaronson KD, Conte JV, Naka Y, Mancini D, Delgado RM, MacGillivray TE, Farrar DJ, Frazier OH. Use of a continuous‐flow device in patients awaiting heart transplantation. N Engl J Med. 2007; 357: 885–896. - PubMed
-
- Slaughter MS, Rogers JG, Milano CA, Russell SD, Conte JV, Feldman D, Sun B, Tatooles AJ, Delgado RM III, Long JW, Wozniak TC, Ghumman W, Farrar DJ, Frazier OH. Advanced heart failure treated with continuous‐flow left ventricular assist device. N Engl J Med. 2009; 361: 2241–2251. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
