

Pre- and post-treatment blood-based genomic landscape of patients with ROS1 or NTRK fusion-positive solid tumours treated with entrectinib
- PMID: 35338679
- PMCID: PMC9120896
- DOI: 10.1002/1878-0261.13214
Pre- and post-treatment blood-based genomic landscape of patients with ROS1 or NTRK fusion-positive solid tumours treated with entrectinib
Abstract
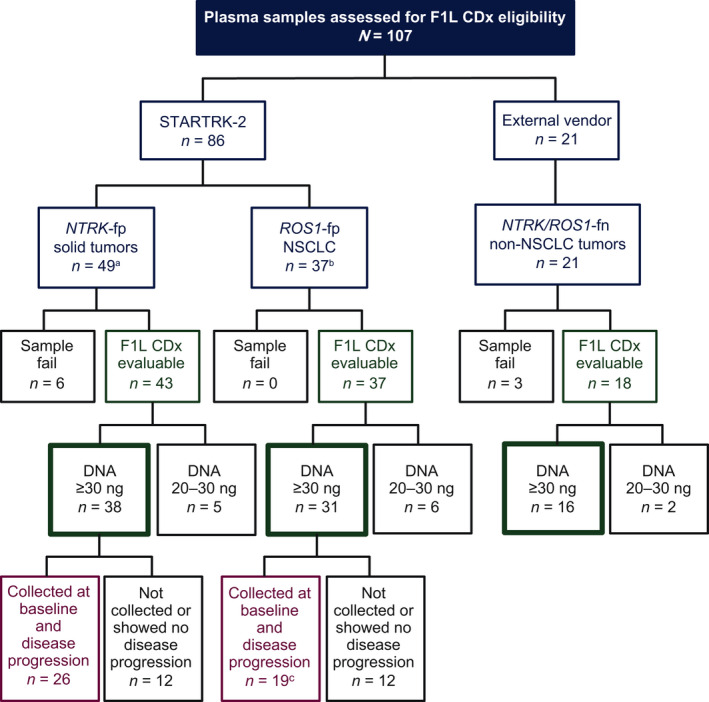
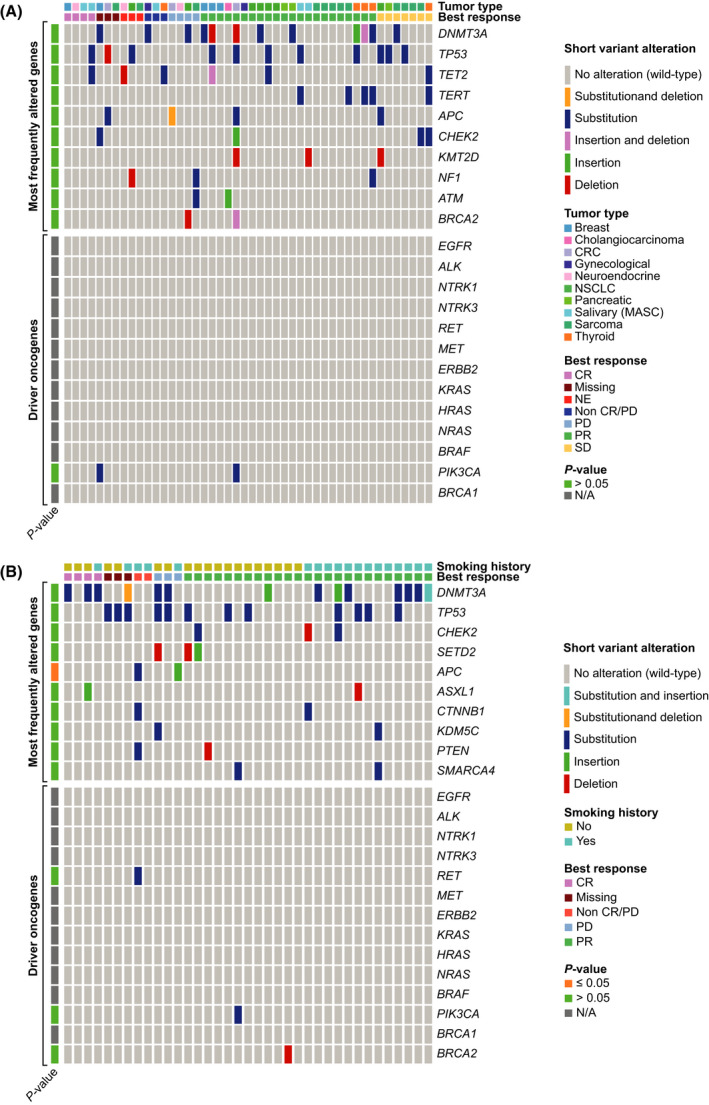
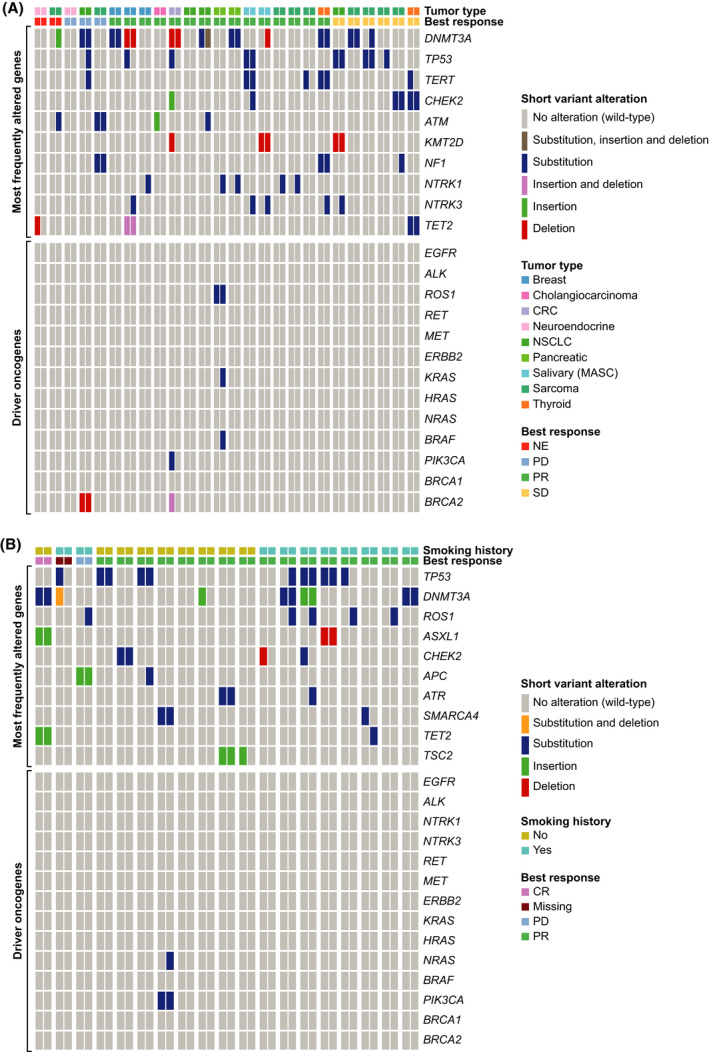
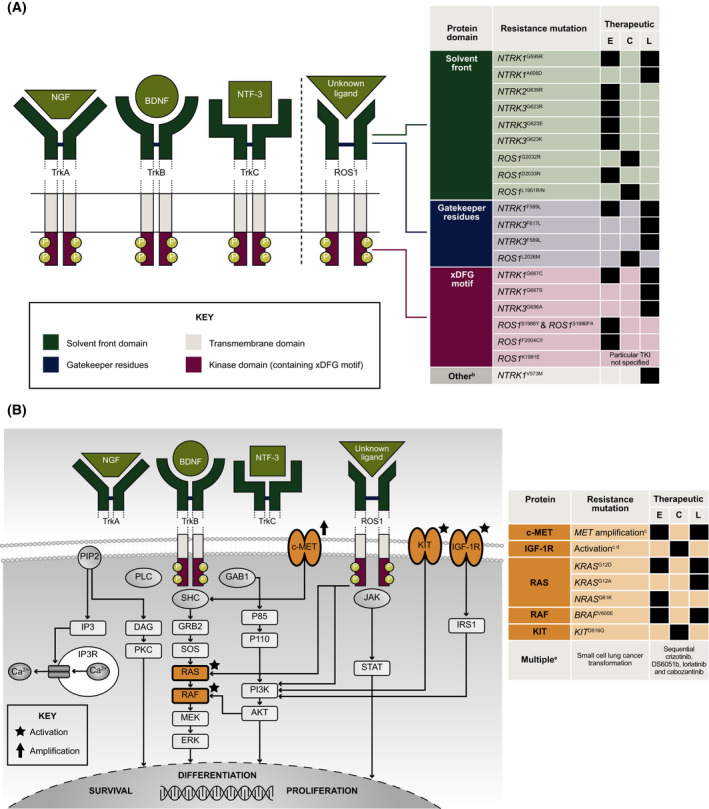
Genomic tumour profiling informs targeted treatment options. Entrectinib is a tyrosine kinase inhibitor with efficacy in NTRK fusion-positive (-fp) solid tumours and ROS1-fp non-small cell lung cancer. FoundationOne® Liquid CDx (F1L CDx), a non-invasive in vitro next-generation sequencing (NGS)-based diagnostic, detects genomic alterations in plasma circulating tumour DNA (ctDNA). We evaluated the clinical validity of F1L CDx as an aid in identifying patients with NTRK-fp or ROS1-fp tumours and assessed the genomic landscape pre- and post-entrectinib treatment. Among evaluable pre-treatment clinical samples (N = 85), positive percentage agreements between F1L CDx and clinical trial assays (CTAs) were 47.4% (NTRK fusions) and 64.5% (ROS1 fusions); positive predictive value was 100% for both. The objective response rate for CTA+ F1L CDx+ patients was 72.2% in both cohorts. The median duration of response significantly differed between F1L CDx+ and F1L CDx- samples in ROS1-fp (5.6 vs. 17.3 months) but not NTRK-fp (9.2 vs. 12.9 months) patients. Fifteen acquired resistance mutations were detected. We conclude that F1L CDx is a clinically valid complement to tissue-based testing to identify patients who may benefit from entrectinib and those with acquired resistance mutations associated with disease progression.
Keywords: NTRK; ROS1; F1L CDx; genomic profiling; resistance.
© 2022 Genentech, Inc. Molecular Oncology published by John Wiley & Sons Ltd on behalf of Federation of European Biochemical Societies.
Conflict of interest statement
The authors declare the following competing financial interests: RD has received consultancy/advisory fees from F. Hoffmann‐La Roche Ltd, Foundation Medicine Inc., Pfizer, AstraZeneca, Celon Pharma, Bristol‐Myers Squibb, Merck, MSD, Regeneron, Takeda, Seattle Genetics, Novartis; and has received travel or accommodation expenses from F. Hoffmann‐La Roche Ltd and AstraZeneca. TH, VC, CW, CWC, BS, and TR are employees of Genentech, Inc. AD reports honoraria/advisory fees from Ignyta/Genentech, Inc./F. Hoffmann‐La Roche Ltd, Loxo/Bayer/Lilly, Takeda/Ariad/Millenium, TP Therapeutics, AstraZeneca, Pfizer, Blueprint Medicines, Helsinn, Beigene, BergenBio, Hengrui Therapeutics, Exelixis, Tyra Biosciences, Verastem, MORE Health, Abbvie, 14ner/Elevation Oncology, Remedica Ltd, ArcherDX, Monopteros, Novartis, EMD Serono, Melendi, Liberum, Repare RX, Nuvalent, Merus; research grant/funding (institution) from Pfizer, Exelixis, GlaxoSmithKlein, Teva, Taiho, PharmaMar; research grant (self) from Foundation Medicine; royalties from Wolters Kluwer; expenses from Merck, Puma, Merus, Boehringer Ingelheim; CME honoraria from Medscape, OncLive, PeerVoice, Physicians Education Resources, Targeted Oncology, Research to Practice, Axis, Peerview Institute, Paradigm Medical Communications, WebMD, MJH Life Sciences, Med Learning, Imedex, Answers in CME, Clinical Care Options. RCD declares consulting fees from Ignyta, Genentech, Inc./F. Hoffmann‐La Roche Ltd, AstraZeneca, Anchiano, and Rain Therapeutics; royalties or licensing fees for intellectual property from Ignyta, Abbott Molecular, Genentech, Inc./F. Hoffmann‐La Roche Ltd, Foundation Medicine, Black Diamond, Pearl River, Voronoi, Takeda, Scorpion, and Rain Therapeutics; stock ownership in Rain Therapeutics; is an employee of Rain Therapeutics. FB reports consulting/advisory role for F. Hoffmann‐La Roche Ltd/Genentech, Inc., Pfizer, Novartis, Pierre Fabre, Bristol‐Myers Squibb, AstraZeneca/MedImmune, Boehringer Ingelheim, Lilly, Merck Serono, MSD Oncology, Takeda, Bayer; travel/accommodation/expenses from F. Hoffmann‐La Roche Ltd/Genentech, Inc., Bristol‐Myers Squibb, AstraZeneca/MedImmune, MSD Oncology; honoraria from F. Hoffmann‐La Roche Ltd/Genentech, Inc., Pfizer, Pierre Fabre, AstraZeneca, Bristol‐Myers Squibb, Boehringer Ingelheim, Lilly, Novartis, Pierre Fabre, Merck Serono, MSD Oncology, Takeda, Bayer; research funding (institution) from F. Hoffmann‐La Roche Ltd/Genentech, Inc., AstraZeneca/MedImmune, Bristol‐Myers Squibb, Pierre Fabre, Abbvie, Amgen, Bayer, Boehringer Ingelheim, Eisai, Lilly, Ipsen, Innate Pharma, Novartis, Merck Serono, MSD Oncology, Pfizer, Sanofi/Aventis, Takeda. TRW is an employee of Genentech, Inc., and has stock and ownership interest in F. Hoffmann‐La Roche Ltd. KW was an employee of Foundation Medicine, Inc. at the time of the study but is now an employee of the US Food and Drug Administration. JS, LD, RW, and ML are employees of Foundation Medicine, Inc.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
