

Exploration of predictive biomarkers for postoperative recurrence of stage II/III colorectal cancer using genomic sequencing
- PMID: 35343095
- PMCID: PMC9487878
- DOI: 10.1002/cam4.4710
Exploration of predictive biomarkers for postoperative recurrence of stage II/III colorectal cancer using genomic sequencing
Abstract
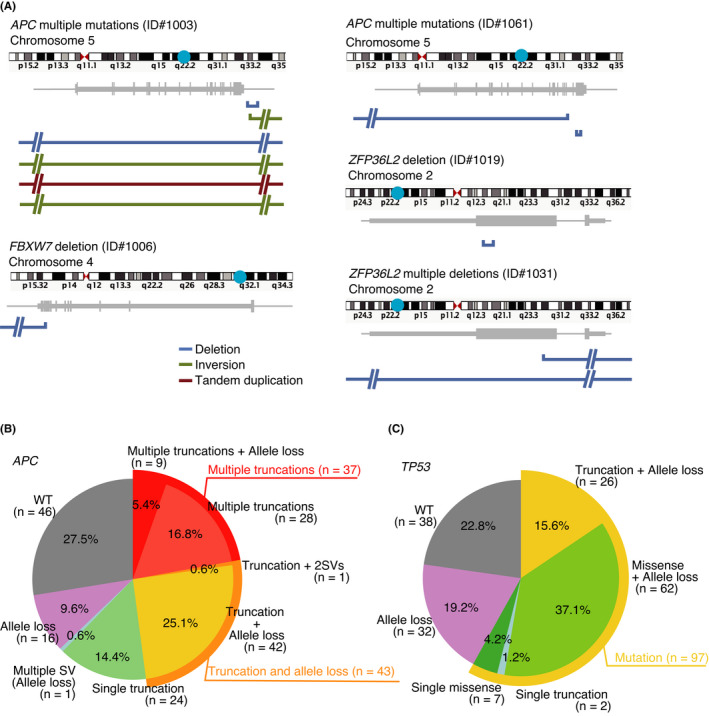
Postoperative recurrence of colorectal cancer (CRC) eventually leads to therapeutic failure; therefore, treatment strategies based on accurate prediction of recurrence are urgently required. To identify biomarkers that can predict treatment outcomes, we compared the mutational profiles of surgically resected specimens from patients with recurrent cancer with those from patients with non-recurrent cancer. Target sequencing, whole-exome sequencing (WES), or whole-genome sequencing (WGS) was performed on 89 and 58 tumors from recurrent and non-recurrent cases, respectively. WGS revealed the driver mutations that were not detected with target sequencing or WES, including the structural variations affecting ZFP36L2. Loss of function of ZFP36L2 was frequently observed in primary tumors from recurrent cases. Furthermore, the recurrence-free survival of patients with loss of function of ZFP36L2 was significantly shorter relative to patients with no loss of ZFP36L2 function. In summary, the study demonstrated that detailed genomic analysis could help improve precision medicine for CRC.
Keywords: ZFP36L2; colorectal cancer; precision medicine; whole genome sequence.
© 2022 The Authors. Cancer Medicine published by John Wiley & Sons Ltd.
Conflict of interest statement
All the authors declare that they have no competing interests.
Figures





References
-
- Gill S, Loprinzi CL, Sargent DJ, et al. Pooled analysis of fluorouracil‐based adjuvant therapy for stage II and III colon cancer: who benefits and by how much? J Clin Oncol. 2004;22:1797‐1806. - PubMed
-
- Figueredo A, Charette ML, Maroun J, Brouwers MC, Zuraw L. Adjuvant therapy for stage II colon cancer: a systematic review from the Cancer Care Ontario program in evidence‐based Care's gastrointestinal cancer disease site group. J Clin Oncol. 2004;22:3395‐3407. - PubMed
-
- Kannarkatt J, Joseph J, Kurniali PC, al‐Janadi A, Hrinczenko B. Adjuvant chemotherapy for stage II colon cancer: a clinical dilemma. J Oncol Pract. 2017;13:233‐241. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
