

Suspicion, screening, and diagnosis of wild-type transthyretin amyloid cardiomyopathy: a systematic literature review
- PMID: 35343098
- PMCID: PMC9065854
- DOI: 10.1002/ehf2.13884
Suspicion, screening, and diagnosis of wild-type transthyretin amyloid cardiomyopathy: a systematic literature review
Abstract
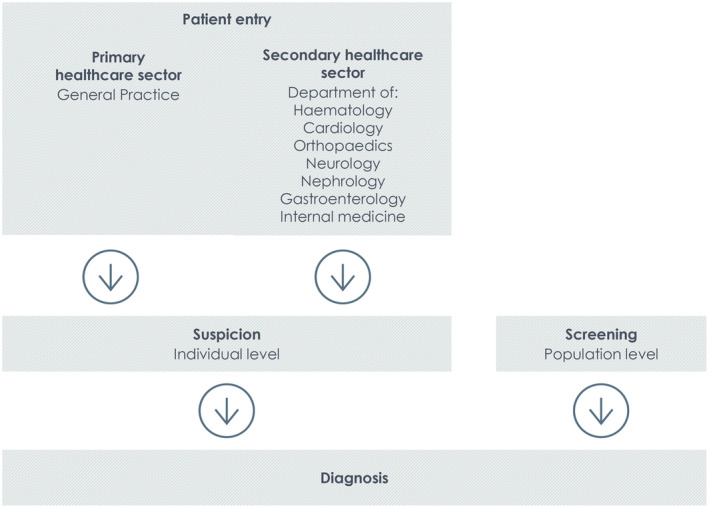
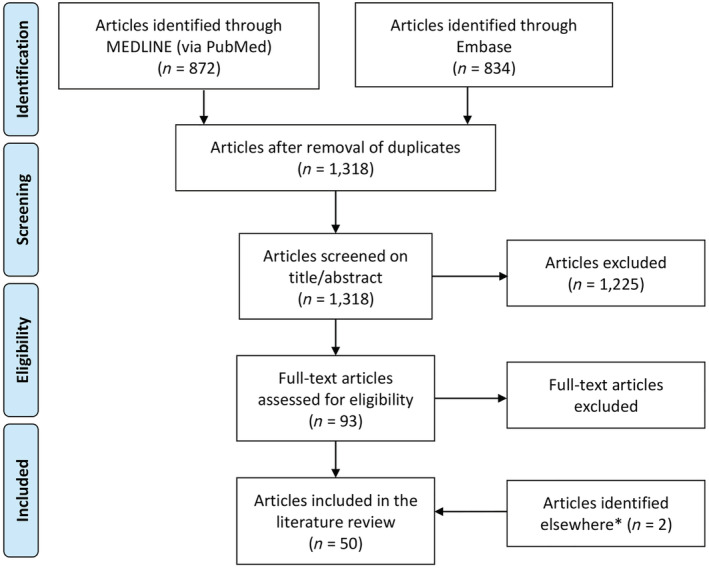
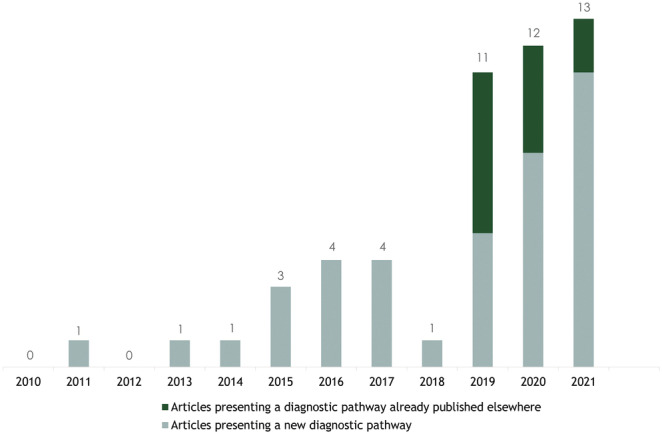
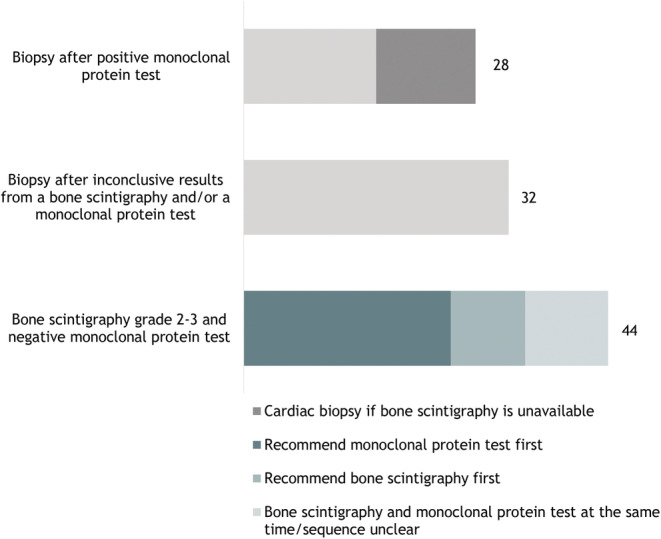
Wild-type transthyretin amyloid cardiomyopathy (ATTRwt CM) is a more common disease than previously thought. Awareness of ATTRwt CM and its diagnosis has been challenged by its unspecific and widely distributed clinical manifestations and traditionally invasive diagnostic tools. Recent advances in echocardiography and cardiac magnetic resonance (CMR), non-invasive diagnosis by bone scintigraphy, and the development of disease-modifying treatments have resulted in an increased interest, reflected in multiple publications especially during the last decade. To get an overview of the scientific knowledge and gaps related to patient entry, suspicion, diagnosis, and systematic screening of ATTRwt CM, we developed a framework to systematically map the available evidence of (i) when to suspect ATTRwt CM in a patient, (ii) how to diagnose the disease, and (iii) which at-risk populations to screen for ATTRwt CM. Articles published between 2010 and August 2021 containing part of or a full diagnostic pathway for ATTRwt CM were included. From these articles, data for patient entry, suspicion, diagnosis, and screening were extracted, as were key study design and results from the original studies referred to. A total of 50 articles met the inclusion criteria. Of these, five were position statements from academic societies, while one was a clinical guideline. Three articles discussed the importance of primary care providers in terms of patient entry, while the remaining articles had the cardiovascular setting as point of departure. The most frequently mentioned suspicion criteria were ventricular wall thickening (44/50), carpal tunnel syndrome (42/50), and late gadolinium enhancement on CMR (43/50). Diagnostic pathways varied slightly, but most included bone scintigraphy, exclusion of light-chain amyloidosis, and the possibility of doing a biopsy. Systematic screening was mentioned in 16 articles, 10 of which suggested specific at-risk populations for screening. The European Society of Cardiology recommends to screen patients with a wall thickness ≥12 mm and heart failure, aortic stenosis, or red flag symptoms, especially if they are >65 years. The underlying evidence was generally good for diagnosis, while significant gaps were identified for the relevance and mutual ranking of the different suspicion criteria and for systematic screening. Conclusively, patient entry was neglected in the reviewed literature. While multiple red flags were described, high-quality prospective studies designed to evaluate their suitability as suspicion criteria were lacking. An upcoming task lies in defining and evaluating at-risk populations for screening. All are steps needed to promote early detection and diagnosis of ATTRwt CM, a prerequisite for timely treatment.
Keywords: ATTRwt CM; Amyloidosis; Cardiomyopathy; Diagnosis; Screening; Suspicion; Transthyretin.
© 2022 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
K.B. was a paid consultant to Pfizer in connection with the development of this manuscript and reports financial relationships outside of the submitted work with Pfizer Denmark. F.G., M.M., and S.H.P. did not receive any funding from Pfizer to conduct this study and have paid for their own work in this project, albeit they report financial relationships outside of the submitted work with Pfizer Denmark. A.B.‐B., A.M.S., and T.P. are employees at Pfizer Denmark.
Figures
References
-
- González‐López E, Gallego‐Delgado M, Guzzo‐Merello G, de Haro‐del Moral FJ, Cobo‐Marcos M, Robles C, Bornstein B, Salas C, Lara‐Pezzi E, Alonso‐Pulpon L, Garcia‐Pavia P. Wild‐type transthyretin amyloidosis as a cause of heart failure with preserved ejection fraction. Eur Heart J 2015; 36: 2585–2594. - PubMed
-
- Yilmaz A, Bauersachs J, Bengel F, Büchel R, Kindermann I, Klingel K, Knebel F, Meder B, Morbach C, Nagel E, Schulze‐Bahr E, aus dem Siepen F, Frey N. Diagnosis and treatment of cardiac amyloidosis: position statement of the German Cardiac Society (DGK). Clin Res Cardiol 2021; 110: 479–506. - PMC - PubMed
-
- González‐López E, Gagliardi C, Dominguez F, Quarta CC, de Haro‐del Moral FJ, Milandri A, Salas C, Cinelli M, Cobo‐Marcos M, Lorenzini M, Lara‐Pezzi E, Foffi S, Alonso‐Pulpon L, Rapezzi C, Garcia‐Pavia P. Clinical characteristics of wild‐type transthyretin cardiac amyloidosis: disproving myths. Eur Heart J 2017; 38: 1895–1904. - PubMed
-
- Witteles RM, Bokhari S, Damy T, Elliott PM, Falk RH, Fine NM, Gospodinova M, Obici L, Rapezzi C, Garcia‐Pavia P. Screening for transthyretin amyloid cardiomyopathy in everyday practice. JACC Heart Fail 2019; 7: 709–716. - PubMed
-
- Gertz M, Adams D, Ando Y, Beirão JM, Bokhari S, Coelho T, Comenzo RL, Damy T, Dorbala S, Drachman BM, Fontana M, Gillmore JD, Grogan M, Hawkins PN, Lousada I, Kristen AV, Ruberg FL, Suhr OB, Maurer MS, Nativi‐Nicolau J, Quarta CC, Rapezzi C, Witteles R, Merlini G. Avoiding misdiagnosis: expert consensus recommendations for the suspicion and diagnosis of transthyretin amyloidosis for the general practitioner. BMC Fam Pract 2020; 21: 198. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous