Comparison of 3 Different Minimally Invasive Surgical Techniques for Lumbar Spinal Stenosis: A Randomized Clinical Trial
- PMID: 35344046
- PMCID: PMC8961320
- DOI: 10.1001/jamanetworkopen.2022.4291
Comparison of 3 Different Minimally Invasive Surgical Techniques for Lumbar Spinal Stenosis: A Randomized Clinical Trial
Abstract
Importance: Operations for lumbar spinal stenosis is the most often performed surgical procedure in the adult lumbar spine. This study reports the clinical outcome of the 3 most commonly used minimally invasive posterior decompression techniques.
Objective: To compare the effectiveness of 3 minimally invasive posterior decompression techniques for lumbar spinal stenosis.
Design, setting, and participants: This randomized clinical trial used a parallel group design and included patients with symptomatic and radiologically verified lumbar spinal stenosis without degenerative spondylolisthesis. Patients were enrolled between February 2014 and October 2018 at the orthopedic and neurosurgical departments of 16 Norwegian public hospitals. Statistical analysis was performed in the period from May to June 2021.
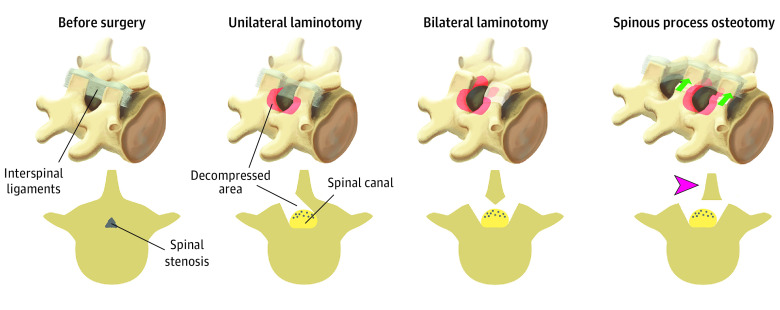
Interventions: Patients were randomized to undergo 1 of the 3 minimally invasive posterior decompression techniques: unilateral laminotomy with crossover, bilateral laminotomy, and spinous process osteotomy.
Main outcomes and measures: Primary outcome was change in disability measured with Oswestry Disability Index (ODI; range 0-100), presented as mean change from baseline to 2-year follow-up and proportions of patients classified as success (>30% reduction in ODI). Secondary outcomes were mean change in quality of life, disease-specific symptom severity measured with Zurich Claudication Questionnaire (ZCQ), back pain and leg pain on a 10-point numeric rating score (NRS), patient perceived benefit of the surgical procedure, duration of the surgical procedure, blood loss, perioperative complications, number of reoperations, and length of hospital stay.
Results: In total, 437 patients were included with a median (IQR) age of 68 (62-73) years and 230 men (53%). Of the included patients, 146 were randomized to unilateral laminotomy with crossover, 142 to bilateral laminotomy, and 149 to spinous process osteotomy. The unilateral laminotomy with crossover group had a mean change of -17.9 ODI points (95% CI, -20.8 to -14.9), the bilateral laminotomy group had a mean change of -19.7 ODI points (95% CI, -22.7 to -16.8), and the spinous process osteotomy group had a mean change of -19.9 ODI points (95% CI, -22.8 to -17.0). There were no significant differences in primary or secondary outcomes among the 3 surgical procedures, except a longer duration of the surgical procedure in the bilateral laminotomy group.
Conclusions and relevance: No differences in clinical outcomes or complication rates were found among the 3 minimally invasive posterior decompression techniques used to treat patients with lumbar spinal stenosis.
Trial registration: ClinicalTrials.gov Identifier: NCT02007083.
Conflict of interest statement
Figures