

Society of Skeletal Radiology- white paper. Guidelines for the diagnostic management of incidental solitary bone lesions on CT and MRI in adults: bone reporting and data system (Bone-RADS)
- PMID: 35344076
- PMCID: PMC9283187
- DOI: 10.1007/s00256-022-04022-8
Society of Skeletal Radiology- white paper. Guidelines for the diagnostic management of incidental solitary bone lesions on CT and MRI in adults: bone reporting and data system (Bone-RADS)
Abstract
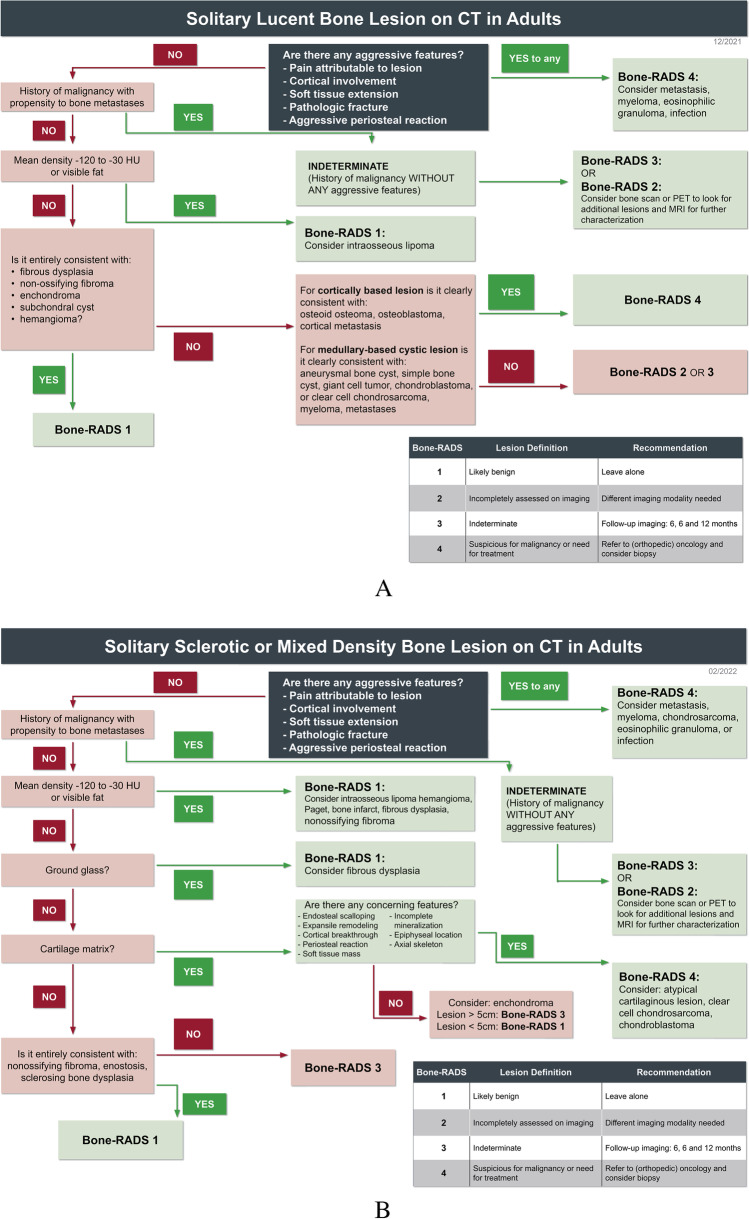
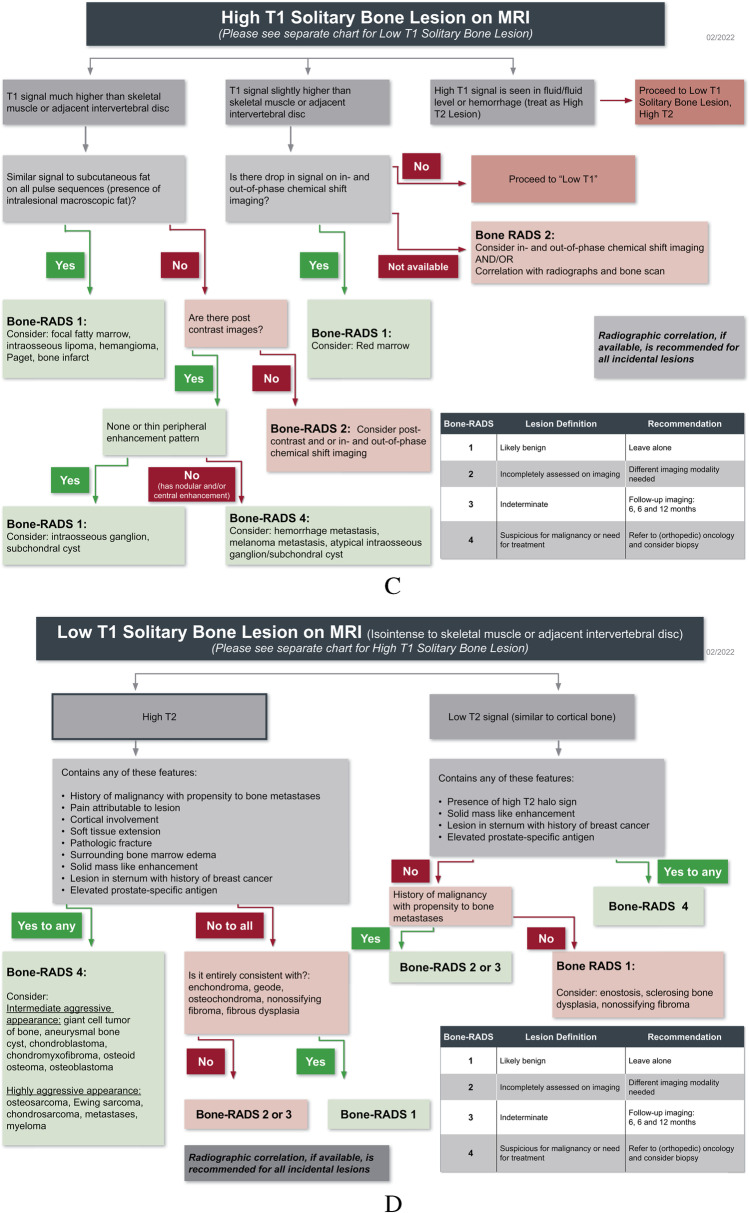
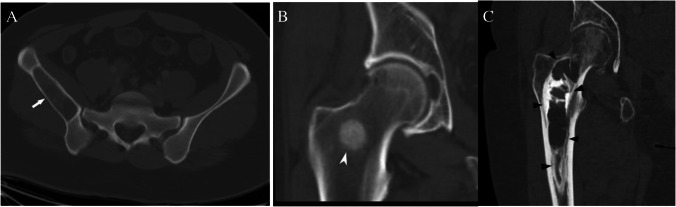
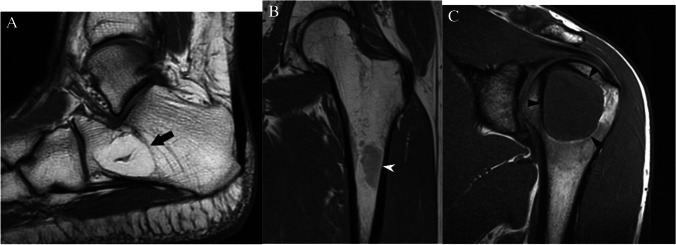
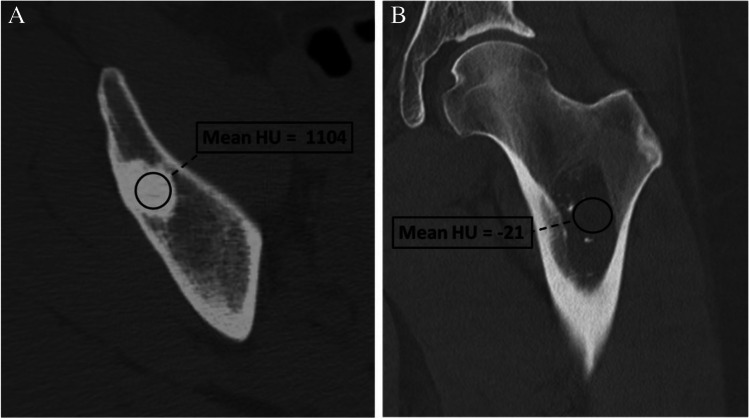
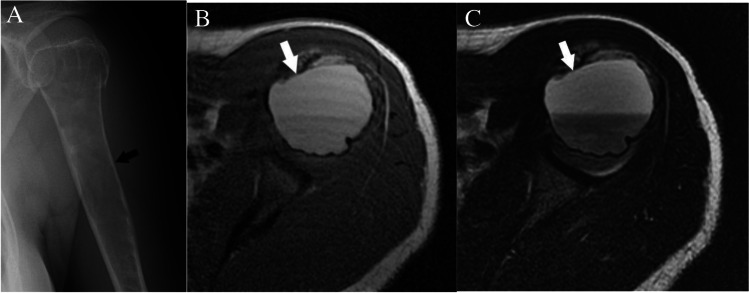
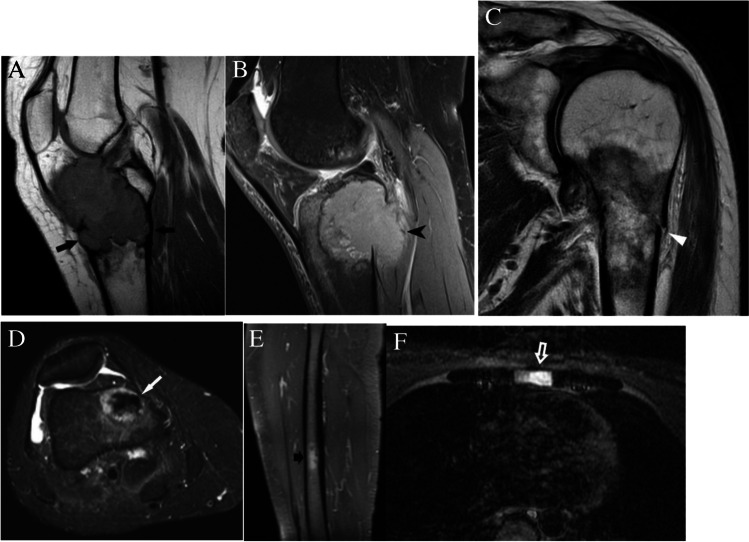
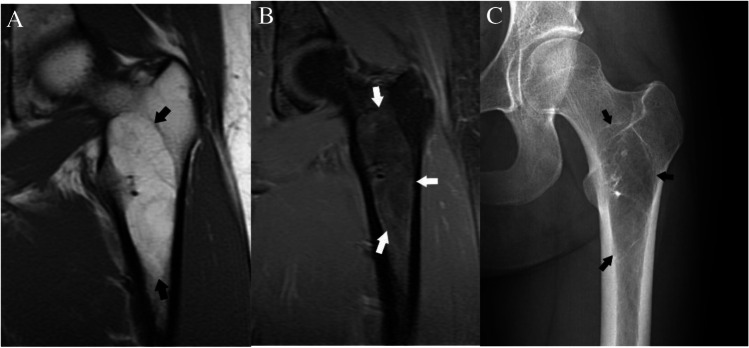
The purpose of this article is to present algorithms for the diagnostic management of solitary bone lesions incidentally encountered on computed tomography (CT) and magnetic resonance (MRI) in adults. Based on review of the current literature and expert opinion, the Practice Guidelines and Technical Standards Committee of the Society of Skeletal Radiology (SSR) proposes a bone reporting and data system (Bone-RADS) for incidentally encountered solitary bone lesions on CT and MRI with four possible diagnostic management recommendations (Bone-RADS1, leave alone; Bone-RADS2, perform different imaging modality; Bone-RADS3, perform follow-up imaging; Bone-RADS4, biopsy and/or oncologic referral). Two algorithms for CT based on lesion density (lucent or sclerotic/mixed) and two for MRI allow the user to arrive at a specific Bone-RADS management recommendation. Representative cases are provided to illustrate the usability of the algorithms.
Keywords: Bone tumors; CT; MRI; Management.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Musculoskeletal Tumor Society: systematic literature review on the use of imaging prior to referral to a musculoskeletal oncologist. Rosemont, IL, Musculoskeletal Tumor Society, February 2018. [Internet]. Available from: http://msts.org/view/download.php/education/pdfs/use-of-imaging-prior-to...
-
- Madewell JE, Ragsdale BD, Sweet DE. Radiologic and pathologic analysis of solitary bone lesions. Part I: internal margins. Radiol Clin North Am. 1981;19:715–48. - PubMed
-
- Ragsdale BD, Madewell JE, Sweet DE. Radiologic and pathologic analysis of solitary bone lesions. Part II: periosteal reactions. Radiol Clin North Am. 1981;19:749–83. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
