

Comorbidities in hereditary angioedema-A population-based cohort study
- PMID: 35344299
- PMCID: PMC8967273
- DOI: 10.1002/clt2.12135
Comorbidities in hereditary angioedema-A population-based cohort study
Abstract
Background: In hereditary angioedema (HAE), low levels (type 1) or defect in function (type 2) of the serine-protease inhibitor C1 Inhibitor protein results in activation of the classical pathway of the complement system as well as the contact system. Here, we investigated the risk of comorbidities in HAE.
Methods: Individuals with HAE (n = 239; identified through a physician made diagnosis) and a control cohort from the general population (n = 2383; matched for age, gender, and county of residence) were compared with the Swedish inpatient, cause of death, cancer, and prescription registers. Conditional logistic regression was used to analyze the data.
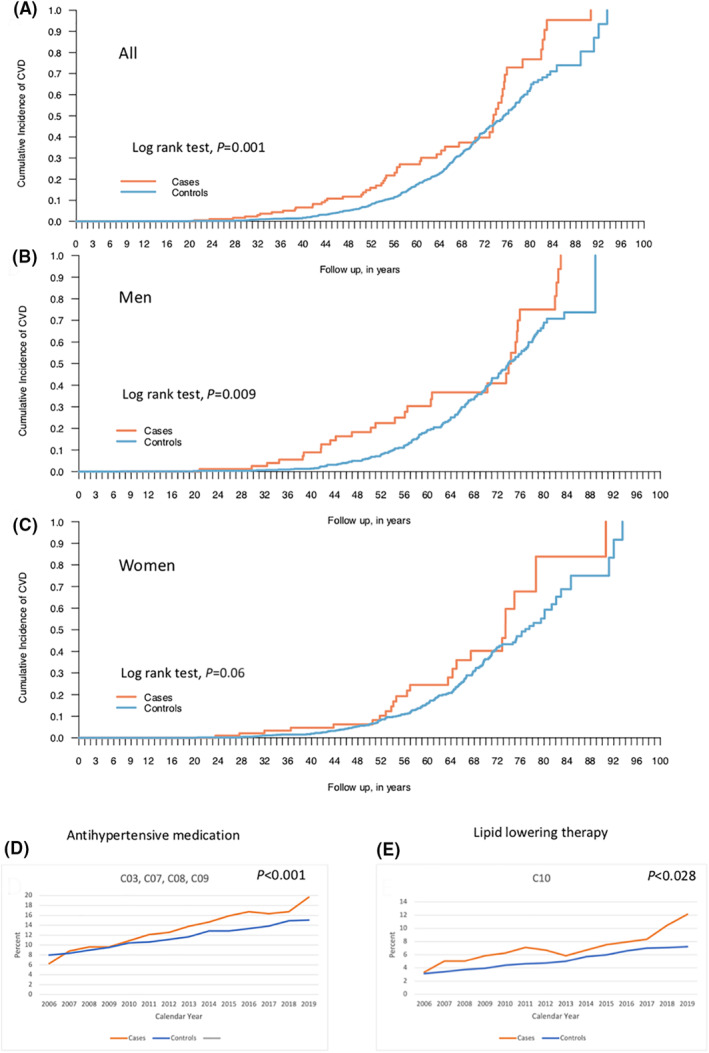
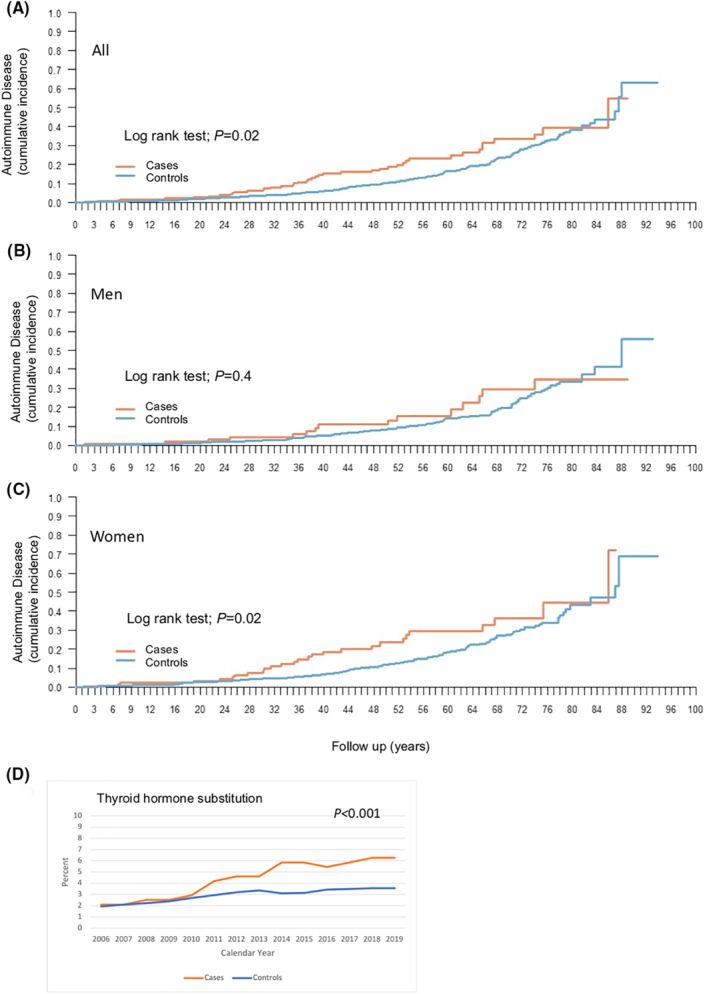
Results: Increased risk of cardiovascular disease (odds ratio [OR] 1.83; 95% confidence interval [CI] 1.32-2.54), including arterial (OR 6.74; 95% CI 1.89-24.06) and venous thromboembolic disease (OR 4.20; 95% CI 2.42-7.23) as well as hypertension (OR 1.64; 95% CI 1.12-2.39) was seen in HAE. There was also an increased number of individuals diagnosed with hyperlipidemia (OR 2.01; 95% CI 1.16-3.50) among HAE patients. Furthermore, the risk of autoimmune disease was increased (OR 1.65; 95% CI 1.15-2.35) being particularly pronounced for systemic lupus erythematosus (OR 71.87; 95% CI 8.80-586.7). The risk of having two or more autoimmune diseases was also higher among HAE patients (p = 0.017). In contrast, the risk of cancer was not increased. Data from the prescription register revealed higher prescription rates of drugs against hypertension, hypothyroidism, and hyperlipidemia among HAE patients.
Conclusions: The results warrant for awareness and prevention of comorbid conditions, in particular, thromboembolic and autoimmune diseases in HAE. Future prophylactic interventions may modify these risks.
Keywords: autoimmunity; cardiovascular disease; complement; epidemiology; hereditary angioedema (HAE).
© 2022 The Authors. Clinical and Translational Allergy published by John Wiley and Sons Ltd on behalf of European Academy of Allergy and Clinical Immunology.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Donaldson VH, Evans RR. A biochemical abnormality in hereditary angioneurotic edema: absence of serum inhibitor of C′ 1‐esterase. Am J Med. 1963;35:37‐44. - PubMed
-
- Rosen FS, Pensky J, Donaldson V, Charache P. Hereditary angioneurotic edema: two genetic variants. Science. 1965;148(3672):957‐958. - PubMed
-
- Busse PJ, Christiansen SC. Hereditary angioedema. N Engl J Med. 2020;382(12):1136‐1148. - PubMed
-
- Bork K, Hardt J, Witzke G. Fatal laryngeal attacks and mortality in hereditary angioedema due to C1‐INH deficiency. J Allergy Clin Immunol. 2012;130(3):692–697. - PubMed
-
- Cugno M, Cicardi M, Bottasso B, et al. Activation of the coagulation cascade in C1‐inhibitor deficiencies. Blood. 1997;89(9):3213‐3218. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
