

Takotsubo Syndrome: Pathophysiology, Emerging Concepts, and Clinical Implications
- PMID: 35344411
- PMCID: PMC7612566
- DOI: 10.1161/CIRCULATIONAHA.121.055854
Takotsubo Syndrome: Pathophysiology, Emerging Concepts, and Clinical Implications
Erratum in
-
Correction to: Takotsubo Syndrome: Pathophysiology, Emerging Concepts, and Clinical Implications.Circulation. 2022 May 17;145(20):e1053. doi: 10.1161/CIR.0000000000001075. Epub 2022 May 16. Circulation. 2022. PMID: 35576318 No abstract available.
Abstract
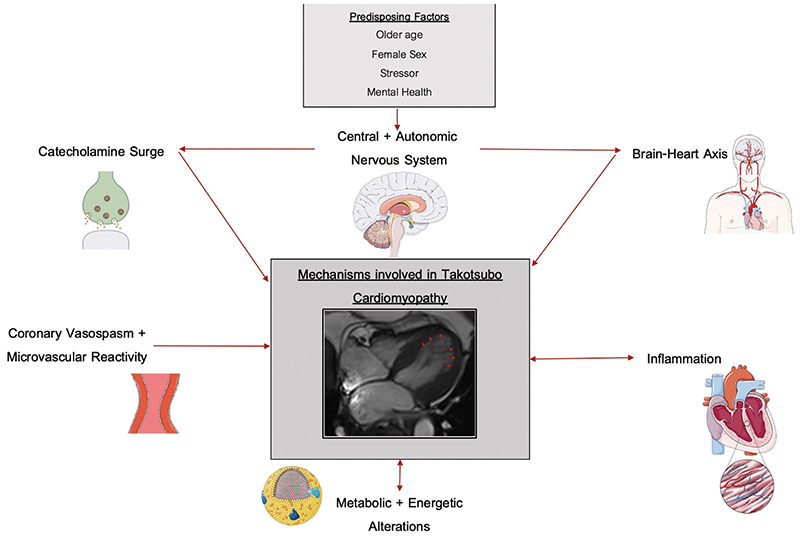
Takotsubo syndrome is a condition characterized by acute transient left ventricular systolic dysfunction, which at presentation can be challenging to distinguish from acute myocardial infarction. Although previously thought to be a benign, self-limiting condition, recent studies have confirmed that patients with takotsubo syndrome have persistent subtle ongoing cardiac dysfunction, and many continue to have limiting symptoms despite restoration of left ventricular ejection fraction. Moreover, these patients have a substantial burden of morbidity and mortality, as well, with high rates of subsequent major adverse cardiovascular events that approach those of patients with acute coronary syndrome. The mechanisms behind this condition remain elusive. Despite substantial research, the medical community continues to have an incomplete understanding of its underlying pathogenesis and pathophysiology. Catecholamine-induced myocardial injury is the most established and well-known theory, but this does not explain all the clinical features and presentations of the condition, and numerous other pathways and abnormalities are emerging. Because of the poor understanding of its underlying pathophysiology, there is a lack of evidence-based interventions to treat the acute episode, to avoid recurrences, and to prevent major adverse cardiovascular events. This highlights the need for further research to gain a better understanding of the underlying pathophysiology to inform appropriate randomized controlled trials of interventions targeting the causative pathways. Only then can evidence-based management strategies be established to improve clinical outcomes of this potentially lethal condition.
Keywords: Takotsubo cardiomyopathy; physiopathology; treatment outcomes.
Conflict of interest statement
none
Figures
References
-
- Sato TH, Uchida T, Dote KMI. Tako-tsubo-like left ventricular dysfunction due to multivessel coronary spasm. Kagakuhyoronsha Publishing Co; Tokyo, Japan: 1990. Clinical Aspect of Myocardial Injury: From Ischemia to Heart Failure.
Publication types
MeSH terms
Substances
Grants and funding
- PG/18/35/33786/BHF_/British Heart Foundation/United Kingdom
- PG/15/88/31780/BHF_/British Heart Foundation/United Kingdom
- CS/17/4/32960/BHF_/British Heart Foundation/United Kingdom
- CH/09/002/26360/BHF_/British Heart Foundation/United Kingdom
- MR/T029153/1/MRC_/Medical Research Council/United Kingdom
- PG/17/64/33205/BHF_/British Heart Foundation/United Kingdom
- RG/16/10/32375/BHF_/British Heart Foundation/United Kingdom
- FS/16/39/32174/BHF_/British Heart Foundation/United Kingdom
- FS/RTF/20/30009/BHF_/British Heart Foundation/United Kingdom
- 053862/WT_/Wellcome Trust/United Kingdom
- RE/18/5/34216/BHF_/British Heart Foundation/United Kingdom
- WT103782AIA/WT_/Wellcome Trust/United Kingdom
- NH/19/1/34595/BHF_/British Heart Foundation/United Kingdom
LinkOut - more resources
Full Text Sources
Medical
