

Hematological Changes in the Second Wave of SARS-CoV-2 in North India
- PMID: 35345814
- PMCID: PMC8956484
- DOI: 10.7759/cureus.23495
Hematological Changes in the Second Wave of SARS-CoV-2 in North India
Abstract
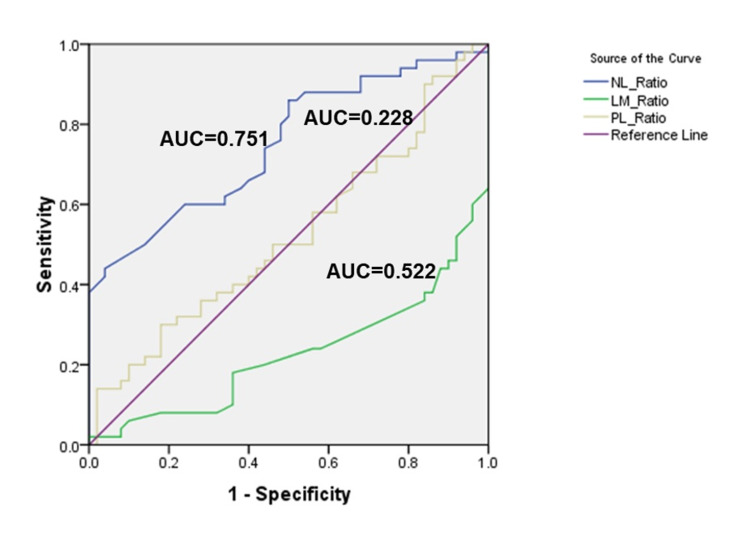
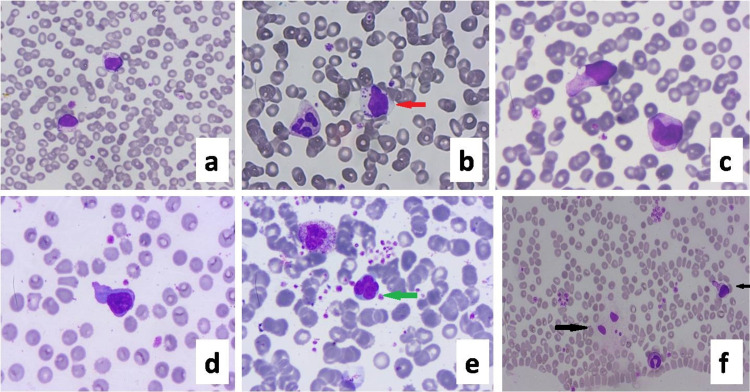
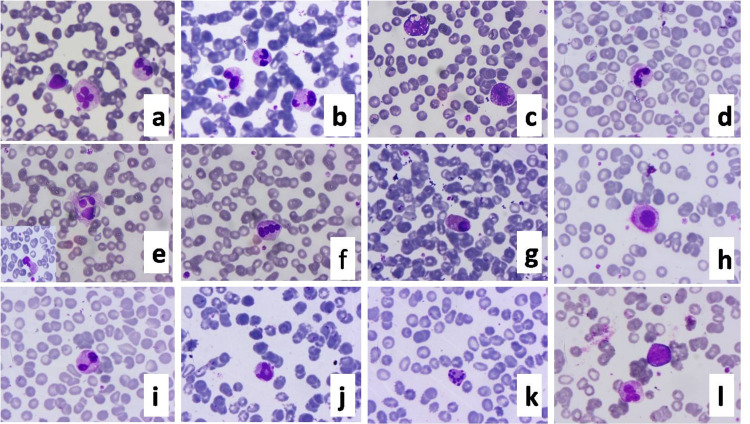
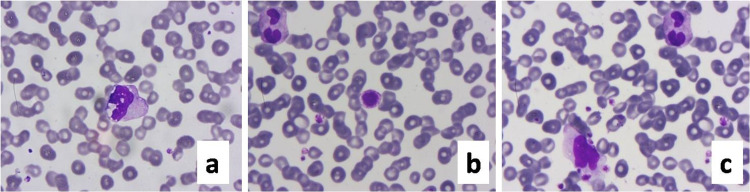
Background COVID-19 is a rapidly spreading pandemic caused by SARS-CoV-2. India experienced a second wave peak in mid of April 2021, and it emerged as a medical crisis. This study was taken up to show if the hematological and peripheral blood changes can be used as a readily available tool to demarcate the patients needing ICU care so that the ICU can be utilized more prudently. Material and method One hundred reverse transcription-polymerase chain reaction (RT-PCR) confirmed cases of COVID-19, 50 each from ICU and non-ICU wards, were included in this observational study. At the time of admission blood sample was collected for evaluation of hematological parameters. Results We noted that 74% of patients admitted in ICU were males and 28% were more than 60 years of age. In ICU patients, the absolute neutrophil count (ANC) was significantly raised when compared to non-ICU cases (p=0.023). The nadir absolute lymphocyte count (ALC) was 0.11x109/L in ICU patients and 0.95x109/L in non-ICU patients. There was a significant increase in neutrophil-lymphocyte ratio (NLR; p<0.001) in ICU patients with a proposed cut-off value of 7.73. Platelet-lymphocyte ratio (PLR) was also raised in ICU patients; however, this increase was not significant (p= 0.623). The proposed cut-off value of PLR is 126.73. A significant reduction in a lymphocyte-monocyte ratio (LMR) was observed in ICU patients when compared to non-ICU cases (p<0.001). Thrombocytopenia was more commonly seen in ICU patients; however, this was not statistically significant. Viral-induced cytopathic effects like plasmacytoid lymphocytes with cytoplasmic granules, the presence of toxic changes in neutrophils, and large-sized platelets were commonly observed in ICU patients. Conclusion Our results suggest that hematological parameters like ANC, absolute lymphocyte count (ALC), platelet count, NLR, PLR, and peripheral smear changes are simple assessment factors that can serve as indicators for the severity of COVID-19 and will demarcate the patients who need ICU-care. This will help in the judicious use of ICU facilities for patients who are actually in need.
Keywords: covid-19 hematological changes; covid-19 india; covid-19 induced cytopathic changes; neutrophil-to-lymphocyte ratio (nlr); platelet-to-lymphocyte ratio (plr); sars-cov-2 infection; second wave of covid-19.
Copyright © 2022, Singh et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Association of Peripheral Blood Parameters With Outcomes of COVID-19 Infection in a Tertiary Care Setting of Eastern India: An Institute-Based Study.Cureus. 2021 Dec 27;13(12):e20745. doi: 10.7759/cureus.20745. eCollection 2021 Dec. Cureus. 2021. PMID: 35113977 Free PMC article.
-
Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio Can Predict the Severity in COVID-19 Patients from Ethiopia: A Retrospective Study.Int J Gen Med. 2022 Oct 7;15:7701-7708. doi: 10.2147/IJGM.S383558. eCollection 2022. Int J Gen Med. 2022. PMID: 36238542 Free PMC article.
-
Dynamic Profile of Prognostic Hematologic Indicators in Patient Under Intensive Care for COVID-19 Disease: A One-Year Study at a Tertiary Care Centre in South India.Cureus. 2021 Nov 15;13(11):e19585. doi: 10.7759/cureus.19585. eCollection 2021 Nov. Cureus. 2021. PMID: 34926056 Free PMC article.
-
Neutrophil-Lymphocyte Ratio Predicting Case Severity in SARS-CoV-2 Infection: A Review.Cureus. 2022 Sep 29;14(9):e29760. doi: 10.7759/cureus.29760. eCollection 2022 Sep. Cureus. 2022. PMID: 36187170 Free PMC article. Review.
-
A Review of the Hematological Picture of Severe COVID-19 Infection.Cureus. 2025 Feb 9;17(2):e78797. doi: 10.7759/cureus.78797. eCollection 2025 Feb. Cureus. 2025. PMID: 39931501 Free PMC article. Review.
Cited by
-
Clinico-pathological study among COVID-19 patients during the second wave of COVID-19 pandemic in Andaman Nicobar Island- "A retrospective cross-sectional study".J Family Med Prim Care. 2022 Nov;11(11):7113-7119. doi: 10.4103/jfmpc.jfmpc_1106_22. Epub 2022 Dec 16. J Family Med Prim Care. 2022. PMID: 36993058 Free PMC article.
-
Modulation in serum and hematological parameters as a prognostic indicator of COVID-19 infection in hypertension, diabetes mellitus, and different cardiovascular diseases.Front Chem. 2024 Apr 29;12:1361082. doi: 10.3389/fchem.2024.1361082. eCollection 2024. Front Chem. 2024. PMID: 38741671 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Miscellaneous