

Comparison of oscillometric, non-invasive and invasive arterial pressure monitoring in patients undergoing laparoscopic bariatric surgery - a secondary analysis of a prospective observational study
- PMID: 35346046
- PMCID: PMC8962134
- DOI: 10.1186/s12871-022-01619-3
Comparison of oscillometric, non-invasive and invasive arterial pressure monitoring in patients undergoing laparoscopic bariatric surgery - a secondary analysis of a prospective observational study
Abstract
Background: Oscillometric, non-invasive blood pressure measurement (NIBP) is the first choice of blood pressure monitoring in the majority of low and moderate risk surgeries. In patients with morbid obesity, however, it is subject to several limitations. The aim was to compare arterial pressure monitoring by NIBP and a non-invasive finger-cuff technology (Nexfin®) with the gold-standard invasive arterial pressure (IAP).
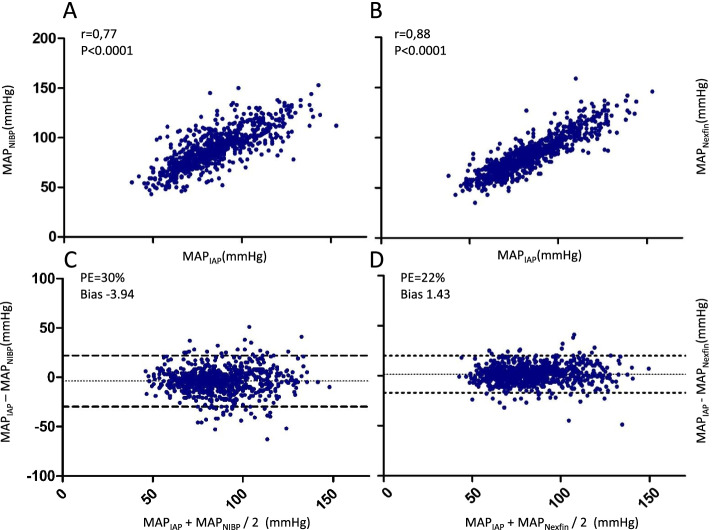
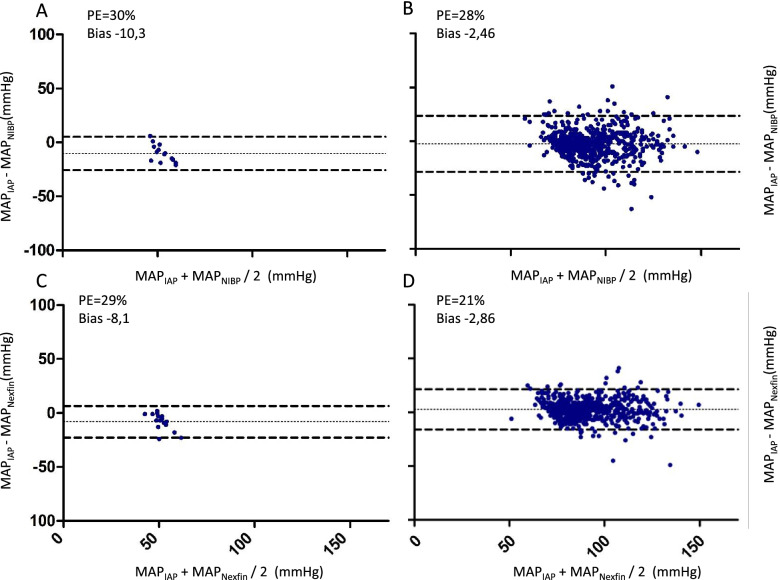
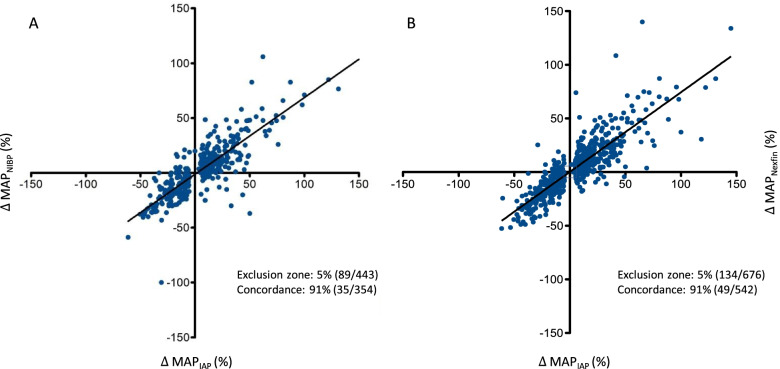
Methods: In this secondary analysis of a prospective observational, single centre cohort study, systolic (SAP), diastolic (DAP) and mean arterial pressure (MAP) were measured at 16 defined perioperative time points including posture changes, fluid bolus administration and pneumoperitoneum (PP) in patients undergoing laparoscopic bariatric surgery. Absolute arterial pressures by NIBP, Nexfin® and IAP were compared using correlation and Bland Altman analyses. Interchangeability was defined by a mean difference ≤ 5 mmHg (SD ≤8 mmHg). Percentage error (PE) was calculated as an additional statistical estimate. For hemodynamic trending, concordance rates were analysed according to the Critchley criterion.
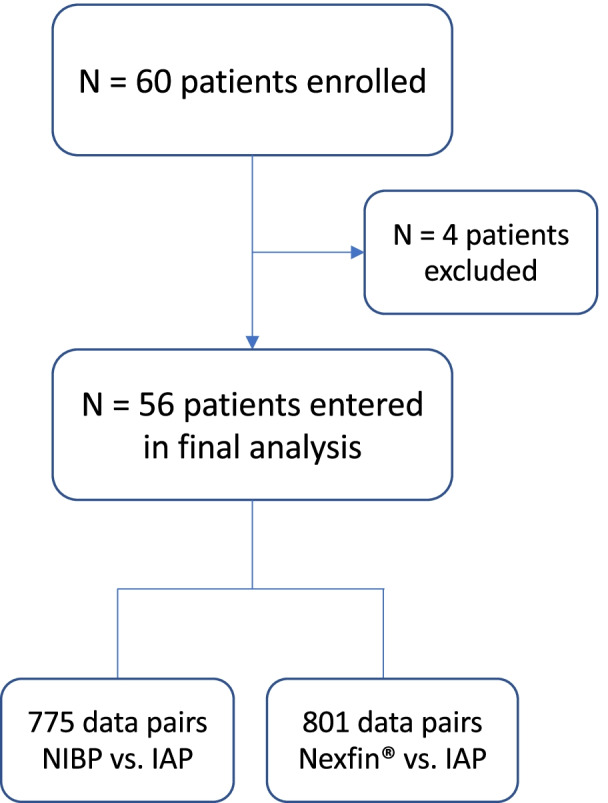
Results: Sixty patients (mean body mass index of 49.2 kg/m2) were enrolled and data from 56 finally analysed. Pooled blood pressure values of all time points showed a significant positive correlation for both NIPB and Nexfin® versus IAP. Pooled PE for NIBP versus IAP was 37% (SAP), 35% (DAP) and 30% (MAP), for Nexfin versus IAP 23% (SAP), 26% (DAP) and 22% (MAP). Correlation of MAP was best and PE lowest before induction of anesthesia for NIBP versus IAP (r = 0.72; PE 24%) and after intraoperative fluid bolus administration for Nexfin® versus IAP (r = 0.88; PE: 17.2%). Concordance of MAP trending was 90% (SAP 85%, DAP 89%) for NIBP and 91% (SAP 90%, DAP 86%) for Nexfin®. MAP trending was best during intraoperative ATP positioning for NIBP (97%) and at induction of anesthesia for Nexfin® (97%).
Conclusion: As compared with IAP, interchangeability of absolute pressure values could neither be shown for NIBP nor Nexfin®, however, NIBP showed poorer overall correlation and precision. Overall trending ability was generally high with Nexfin® surpassing NIBP. Nexfin® may likely render individualized decision-making in the management of different hemodynamic stresses during laparoscopic bariatric surgery, particularly where NIBP cannot be reliably established.
Trial registration: The non-interventional, observational study was registered retrospectively at ( NCT03184285 ) on June 12, 2017.
Keywords: Bariatric surgery; Blood pressure; Clear sight; Finger-cuff; Nexfin; Non-invasive monitoring; Obesity; Vascular unloading technique.
© 2022. The Author(s).
Conflict of interest statement
All authors have provided information on potential conflicts of interests directly or indirectly related to the work submitted. All other authors declared that they have no conflict of interest.
Figures
Similar articles
-
Perioperative non-invasive versus semi-invasive cardiac index monitoring in patients with bariatric surgery - a prospective observational study.BMC Anesthesiol. 2020 Aug 10;20(1):196. doi: 10.1186/s12871-020-01110-x. BMC Anesthesiol. 2020. PMID: 32778047 Free PMC article. Clinical Trial.
-
Comparison of the non-invasive Nexfin® monitor with conventional methods for the measurement of arterial blood pressure in moderate risk orthopaedic surgery patients.J Int Med Res. 2016 Aug;44(4):832-43. doi: 10.1177/0300060516635383. Epub 2016 May 2. J Int Med Res. 2016. PMID: 27142436 Free PMC article. Clinical Trial.
-
Continuous noninvasive monitoring of arterial pressure using the vascular unloading technique in comparison to the invasive gold standard in elderly comorbid patients: A prospective observational study.Health Sci Rep. 2020 Nov 10;3(4):e204. doi: 10.1002/hsr2.204. eCollection 2020 Dec. Health Sci Rep. 2020. PMID: 33204849 Free PMC article.
-
Level of agreement between Nexfin non-invasive arterial pressure with invasive arterial pressure measurements in children.Br J Anaesth. 2012 Oct;109(4):609-15. doi: 10.1093/bja/aes295. Epub 2012 Aug 19. Br J Anaesth. 2012. PMID: 22907342
-
Continuous Non-Invasive Arterial Pressure Assessment during Surgery to Improve Outcome.Front Med (Lausanne). 2017 Nov 17;4:202. doi: 10.3389/fmed.2017.00202. eCollection 2017. Front Med (Lausanne). 2017. PMID: 29204425 Free PMC article. Review.
Cited by
-
Comparing the haemodynamic effects of high- and low-dose opioid anaesthesia: a secondary analysis of a randomised controlled trial.J Clin Monit Comput. 2024 Dec;38(6):1347-1355. doi: 10.1007/s10877-024-01195-6. Epub 2024 Jul 20. J Clin Monit Comput. 2024. PMID: 39031233 Free PMC article. Clinical Trial.
-
Intraoperative haemodynamic monitoring and management of adults having non-cardiac surgery: Guidelines of the German Society of Anaesthesiology and Intensive Care Medicine in collaboration with the German Association of the Scientific Medical Societies.J Clin Monit Comput. 2024 Oct;38(5):945-959. doi: 10.1007/s10877-024-01132-7. Epub 2024 Feb 21. J Clin Monit Comput. 2024. PMID: 38381359 Free PMC article.
-
Blood pressure during ambulation: are noninvasive beat-by-beat finger measures and intermittent brachial measures comparable?Clin Auton Res. 2023 Apr;33(2):197-199. doi: 10.1007/s10286-023-00930-4. Epub 2023 Feb 17. Clin Auton Res. 2023. PMID: 36800050 No abstract available.
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
